
Streptococcus agalactiae: Introduction, Morphology, Pathogenicity, Lab Diagnosis, Treatment, Prevention and Keynotes
Introduction
Streptococcus agalactiae, also known as Group B Streptococcus (GBS), is a gram-positive bacterium that is commonly found in the human gastrointestinal and genital tracts. While it is a normal part of the bacterial flora in these areas, it can also cause infections, especially in newborns and individuals with weakened immune systems.
Streptococcus agalactiae is a leading cause of neonatal sepsis and meningitis, and can also cause infections in pregnant women, elderly individuals, and those with chronic medical conditions. It is typically spread through contact with an infected individual or from mother to baby during childbirth.
GBS screening is recommended for all pregnant women during the third trimester to detect any colonization and take appropriate measures to prevent neonatal infection. Antibiotics can be given during labor to reduce the risk of transmission to the newborn.
Morphology
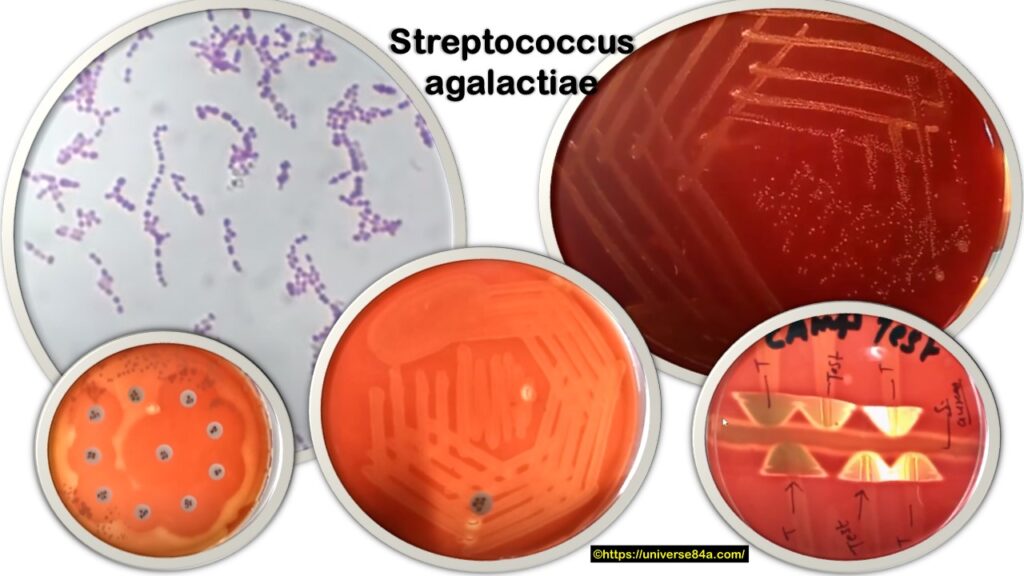
Streptococcus agalactiae is a gram-positive bacterium that appears spherical or oval-shaped under a microscope. Like other streptococci, it is arranged in pairs or chains, with each cell measuring about 0.5 to 1.0 micrometers in diameter.
The cell wall of S. agalactiae contains peptidoglycan, teichoic acids, and lipoteichoic acids, which give the bacterium its characteristic cell shape and also provide protection from the host immune system.
On blood agar plates, S. agalactiae colonies are typically small, gray-white, and slightly raised with a smooth, shiny surface. They also exhibit beta-hemolysis, which means that they completely lyse red blood cells in the surrounding medium.
Pathogenicity
Streptococcus agalactiae is considered a pathogenic bacterium, capable of causing a variety of infections in humans. The following are some of the diseases associated with S. agalactiae:
- Neonatal infections: S. agalactiae is a major cause of neonatal sepsis, pneumonia, and meningitis. Transmission from the mother to the newborn during delivery is the most common mode of transmission.
- Invasive infections in adults: It can cause infections such as bacteremia, endocarditis, pneumonia, and urinary tract infections in adults, particularly in those with underlying medical conditions.
- Skin and soft tissue infections: S. agalactiae can cause skin and soft tissue infections, such as cellulitis and necrotizing fasciitis.
- Bone and joint infections: S. agalactiae can cause osteomyelitis and septic arthritis.
The pathogenicity of S. agalactiae is attributed to several virulence factors, including the capsule, adhesins, and toxins. The capsule protects the bacterium from phagocytosis by the host immune system. Adhesins allow the bacterium to attach to host cells and tissues, while toxins can cause tissue damage and inflammation.
Lab Diagnosis
The laboratory diagnosis of Streptococcus agalactiae involves a combination of techniques to identify and isolate the bacteria.
- Specimen collection: Clinical specimens such as blood, urine, cerebrospinal fluid, and wound swabs are collected from patients suspected of having an S. agalactiae infection.
- Gram stain: A Gram stain of the clinical specimen can help to identify the presence of gram-positive cocci in pairs or chains.
- Culture: Clinical specimens are inoculated onto appropriate culture media, such as blood agar, and incubated at 35-37°C in 5-10% CO2 for 24-48 hours. S. agalactiae typically forms small, gray-white, and slightly raised colonies with smooth, shiny surfaces.
- Biochemical tests: Several biochemical tests can be performed to confirm the identity of S. agalactiae, including catalase, bile esculin, and hippurate hydrolysis tests.
- Serological tests: Serological tests, such as latex agglutination or enzyme-linked immunosorbent assay (ELISA), can be performed to detect the presence of specific S. agalactiae antigens.
- Molecular tests: Molecular methods, such as polymerase chain reaction (PCR), can be used to detect the presence of S. agalactiae DNA in clinical specimens.
Treatment
The treatment of Streptococcus agalactiae infections involves the use of antibiotics. The choice of antibiotic depends on the site and severity of infection, as well as the antibiotic susceptibility of the bacteria.
For neonatal infections, intravenous ampicillin and gentamicin are the drugs of choice, with penicillin as an alternative. For pregnant women colonized with S. agalactiae, intravenous penicillin or ampicillin is given during labor to prevent transmission to the newborn.
For invasive infections in adults, such as bacteremia, endocarditis, and pneumonia, intravenous penicillin or ceftriaxone is often used, with vancomycin reserved for cases of penicillin allergy or resistance.
For skin and soft tissue infections, such as cellulitis and necrotizing fasciitis, penicillin, or clindamycin is typically used.
For bone and joint infections, such as osteomyelitis and septic arthritis, intravenous penicillin or ceftriaxone is usually the first-line treatment, with vancomycin reserved for cases of penicillin allergy or resistance.
It is important to complete the full course of antibiotics to ensure complete eradication of the bacteria and prevent the development of antibiotic resistance. In addition to antibiotics, supportive measures such as wound care, fluids, and pain management may also be necessary for certain infections.
Prevention
The prevention of Streptococcus agalactiae infections involves several strategies aimed at reducing the transmission of the bacteria from colonized individuals to susceptible individuals.
- Screening and treatment of pregnant women: Pregnant women should be screened for S. agalactiae colonization at 35-37 weeks of gestation and given prophylactic antibiotics during labor to prevent transmission to the newborn.
- Universal screening: Some countries have implemented universal screening of pregnant women for S. agalactiae colonization to identify and treat carriers before delivery.
- Contact precautions: Patients with invasive S. agalactiae infections should be placed on contact precautions, including hand hygiene, gloves, and gowns, to prevent transmission to healthcare workers and other patients.
- Vaccination: Efforts are underway to develop a vaccine against S. agalactiae, which could provide protection against neonatal and adult infections.
- Education: Education of healthcare workers and the general public about the risks and prevention of S. agalactiae infections can help to increase awareness and reduce transmission.
By implementing these preventive measures, it is possible to reduce the incidence of S. agalactiae infections and improve outcomes for affected individuals.
Keynotes
- Streptococcus agalactiae is a gram-positive bacterium that is a common cause of neonatal sepsis, meningitis, and pneumonia, as well as infections in pregnant women and immunocompromised adults.
- S. agalactiae is often found in colonizing the genital and gastrointestinal tracts of healthy individuals, and transmission can occur during childbirth, sexual contact, or other routes of exposure.
- Laboratory diagnosis of S. agalactiae involves the collection of appropriate clinical specimens, Gram staining, culture, biochemical tests, serological tests, and molecular tests.
- Treatment of S. agalactiae infections typically involves the use of antibiotics, such as penicillin, ampicillin, or ceftriaxone, with the choice of the drug depending on the site and severity of the infection and the antibiotic susceptibility of the bacteria.
- Prevention of S. agalactiae infections involves strategies such as screening and treatment of pregnant women, universal screening, contact precautions, vaccination, and education of healthcare workers and the general public.
- Accurate identification and prompt treatment of S. agalactiae infections can help to improve outcomes and prevent the spread of infection.
Further Readings
- Colbourn, T., et al. (2017). Prevention of neonatal group B streptococcal disease: a systematic review and meta-analysis. The Lancet Infectious Diseases, 17(8), 863-872.
- Edwards, M. S., & Baker, C. J. (2018). Group B Streptococcal Infections. In Feigin and Cherry’s Textbook of Pediatric Infectious Diseases (8th ed., pp. 1345-1364). Elsevier.
- Khatami, A., et al. (2017). Streptococcus agalactiae: a uropathogen? Journal of global infectious diseases, 9(2), 49-52.
- Kwatra, G., et al. (2017). Epidemiology of invasive group B streptococcal disease in infants from urban area of South Africa, 2003-2013. BMC infectious diseases, 17(1), 1-7.
- Le Doare, K., Heath, P. T., & Sharland, M. (2016). An overview of global GBS epidemiology. Vaccine, 34(26), 2875-2879.
- Puopolo, K. M. (2018). Streptococcus agalactiae (Group B Streptococcus). In Remington and Klein’s Infectious Diseases of the Fetus and Newborn Infant (8th ed., pp. 397-416). Elsevier.
- Schrag, S. J., et al. (2016). Prevention of perinatal group B streptococcal disease—revised guidelines from CDC, 2010. MMWR recommendations and reports, 59(RR-10), 1-36.
- Skoff, T. H., et al. (2019). The global burden of Group B Streptococcus and recommendations for systematic reporting of invasive GBS disease in infants, elderly, and pregnant women in GBS-prevalent settings. The Lancet Infectious Diseases, 19(12), e351-e360.