
Fungal Infections Laboratory Diagnosis: Introduction, Sample Collections and Procedure

Introduction of Fungal infections Laboratory diagnosis
Initially, fungal infections or diseases were neglected but nowadays they are emerging as a huge problem for proper treatment of patients in health care settings and fungal infections are-
The infection of fungi is called mycoses.
Fungal infections are divided into four groups and they are-
- Superficial mycoses: The filamentous fungi which cause superficial disease in humans may be broadly divided into two groups. Primarily the dermatophytes, natural group-related fungi causing the disease tinea or ringworm in various forms. Secondarily a miscellaneous group of unrelated filamentous fungi may be saprophytes or plant pathogens which produce clinical conditions of skin, hair, nail, eye, or ear, causing Tinea Nigra (Hortaea werneckii) , Piedra (Trichosporon and Piedraia hortae), and Malassezia infections.
- Cutaneous mycoses: It is caused by dermatophytes a group of three genera Trichophyton, Microsporum, and Epidermophyton.
- Subcutaneous mycoses: It is localized, spreading infections that result from the inoculation into cutaneous and sub cutaneous tissue of wide of saprophytic fungi are Chromobalstomycosis, Mycetoma, Sporotrichosis, Rhinosporidiosis.
- Systemic mycoses: The fungi which cause the deep or systemic mycoses are Histoplasmosis, Blastomycosis, Cryptococcosis, Coccidioidosis, Paracoccidioidosis.
Pathogenic group of fungi
They are of two types:
- True pathogens and
- Opportunistic pathogens
True pathogens are of four genera
- Histoplasma
- Blastomyces dermatitidis
- Coccidioides immitis
- Paracoccidioides brasiliensis
Opportunistic pathogens are-
- Candida
- Aspergillus
- Pneumocystis jirovecii
- Mucor
- Penicillium
Some fungal diseases and their causative agents

Importance of Fungal infections or diseases and their laboratory Diagnosis
Fungal infections or diseases are difficult to manage because of the following reasons-
- they tend to be chronic,
- hard to diagnose,
- and difficult to eradicate with anti-fungal drugs.
In the near horizon, the prevalence of fungal diseases is likely to increase, as there will be more hosts with impaired immunity and drug resistance will inevitably increase after selection by anti-fungal drug use.
There is a need in progress in the development of new drugs, diagnostics, vaccines, and immunotherapies.
On the far horizon, humanity may face new fungal diseases in association with climate change.
Some current associations between chronic diseases and fungal infections could lead to the establishment of fungi as causative agents, which will not greatly enhance their medical importance but also longer hospital stay and economic burden.
Fungal infections Laboratory diagnosis can be carried out under following points
Specimens
Direct Examination of specimens
Macroscopy
Microscopy (KOH preparation, staining techniques, direct immunofluorescence, and histology)
Culture and isolation
Identification of culture growth
Colony character
Microscopy ( Tease mount, cellophane tape preparation, and slide culture)
Nucleic acid probes
An indirect method based on host immune response
Skin testing
Serological tests
Miscellaneous tests for the identification of yeasts and molds.
General aspects for fungal infection
Specimen
The laboratory diagnosis of a fungal disease starts with the collection of the appropriate specimen. The specimen must contain the viable etiological agent, to be recovered and identified. The anatomical site in which the organism is present must be carefully selected and the specimen collected in such a manner that it will allow the fungus to remain viable in its natural state, with no contamination.
The following are guidelines for specimen collection:
- The specimen should be collected from an active lesion, old ‘burned–out’ lesions often do not contain viable organisms.
- Collect the specimen under aseptic conditions.
- Collect sufficient specimens.
- Collect specimen before initiating therapy.
- Use sterile collection devices and containers
- Label the specimens appropriately.
- All clinical specimens should be considered as potential biohazards and should be handled with care using universal precautions.
Specimen transport and storage for Fungal Infections Laboratory Diagnosis
Except for blood and corneal scrapings, it is not necessary to transport the specimen in a transport medium. The swabs containing specimen for Candida spp. can be transported in a Trichomonas medium containing antibiotics.
Processing of specimens for fungal infections
Processing is necessary to ensure the viability of the etiological agents and to minimize the chances of contamination. Specimens from normally sterile sites need no special processing, if the volume is adequate, specimens should be concentrated by centrifugation. Aseptically collected tissue should be homogenized in a tissue grinder, mortar-pestle. A portion of tissue suspected to contain zygomycetes should be finely minced with a pair of scissors or scalpels. A highly viscous specimen, such as sputum should be liquified.
Culture
For culture, two media are selected. One media will support the growth of any fungus and the other will selectively inhibit contaminating microorganisms.
Media
Fungi will grow on most non-selective culture media, so pathogenic fungi can be recovered from bacteriological media if given enough time to grow. The culture media may be divided into 3 broad categories.
- Non-selective media- It supports the growth of most fungi present in clinical specimens, such as SDA, BHI agar, PDA, etc.
- Selective media- Combinations of antibacterial antibiotics and cycloheximide may be added to these media to make them selective. Selective media may be inhibitory to bacteria only containing antibiotics or inhibitory to both bacteria and fungi containing antibiotics and cycloheximide. 500 µg/ml of cycloheximide & 16 µg/ml of chloramphenicol are added to the fungal culture media. Better results have been achieved using a combination of 5µg/ml of gentamicin and 16 µg/ml of chloramphenicol as an antibacterial agent for fungal culture media. Ciprofloxacin at a concentration of 5 µg/ml may be used.
- Differential media- Many differential media are based on the biochemical reaction which causes the chromogenic substrate or indicator, incorporated into media to show color change or pigment production. For example CHROM agar for Candida spp. and dermatophyte test medium for the dermatophytes.
Incubation conditions
Fungi commonly associated with the disease will grow at temperatures between 25-30⁰C. It is accepted that 30⁰C is the optimal temperature for isolating fungi from clinical specimens. For dimorphic fungi, the culture media are incubated both at 30⁰C for the growth of mold form and 37⁰C for the growth of yeast form. A humid environment is provided to prevent plated media from drying during the incubation period of 4-6 weeks.
Fungal infections can be classified according to the site of involvement as-
Superficial mycoses (Surface and cutaneous mycoses)
Subcutaneous mycoses
Systemic mycoses
Opportunistic mycosesLaboratory diagnosis of superficial mycose
Superficial mycoses are the infection of the superficial layer i.e. keratinized layers of the skin and its appendages and mucosa of the oral cavity and vagina in case of mucosal candidiasis. Etiology – surface mycoses are caused by Malassezia furfur, Exophiala werneckii, Trchosporon beigelli, and Piedraia hortae, and cutaneous mycoses are caused by dermatophytes and in the case of mucosal candidiasis by Candida spp.
Sample collection for superficial mycoses
Samples may be obtained by scraping the skin and nails with a scalpel blade or microscope slide holding at 90 degrees. Skin samples are scraped from the outer edges of the surface lesions. Skin and nails must be cleaned with 70 % isopropanol before sampling. Infected hair should be removed by plucking with forceps and never by cutting because cutting fails to remove the area most likely to harbor the fungus i.e. the base of the hair shaft around the follicle. The collection of hair samples is facilitated by a wood lamp. In the case of onychomycosis, the patient should stop antifungal agents one week prior to the collection of the specimen. Nail specimens should be clipped from the free edge. The fungus in the distal portion of the nail is often non-viable and if the culture does fail samples can be taken from the base of the nail. In the case of superficial candidiasis, the sample is collected by repeatedly rubbing the swab firmly over the white plaques.
Skin stripping
This is an alternative method for the collection of skin specimens. A waterproof transparent adhesive tape is applied firmly to the affected area and peels it off. The tape now bearing a thin layer of skin is then applied to the sterile glass slide with KOH.Hairbrush sampling technique
Hair samples may be collected from the scalp by brushing with a sterile plastic hairbrush or scalp massage pad which is then inoculated into a culture medium by pressing the brush or pad spines into the SDA.
Storage & transport of sample for superficial mycoses
These samples should be allowed to dry out because the moisture causes to overgrow the contaminants. Black paper containing the specimen may be folded to form a packet. In such conditions, ringworm fungi remain viable for weeks or even months(up to 12 months). The specimen should not be refrigerated as the viability of some species(Epidermophyton spp.) is affected. The survival of yeasts on the dry swabs is inversely related to time and storage temperature. In case of delay can be stored at 4⁰C.
Direct Examinations
Direct examination of clinical material provides a rapid report to the physician to initiate the treatment. In some cases, specific morphological characteristics provide a clue to the genus of organisms. It may provide evidence of infection despite negative cultures in the case of antifungal therapy.
Microscopic examination
KOH preparation
Principle- The fungal cell wall glucans being alkali resistant, is not dissolved in KOH and other skin layers, keratin, mucus, and other tissue components are dissolved.
10 or 20 or 30 % KOH is used. Skin, nail, hair, or other samples obtained are mixed with a drop of KOH on a slide and covered with a coverslip. Heat may be applied to potentiate the clearing of tissue. If the specimen is transparent it may be examined without treatment with KOH. Malassezia furfur shows oval or bottle-shaped cells along with short, curved hyphae. Hortae wernecki shows brownish, branched, septate hyphae and budding cells. Trichosporon beigelli shows hyphae and rectangular arthrospores within(endothrix) and around(exothrix) hair. Piedraia hortae shows dark color septate hyphae around hair and asci containing 2-8 aseptate ascospores. Dermatophytes in a skin scraping, nail clippings, or nail scraping and hair stubs can appear as refractile, hyaline, septate, branched, or unbranched hyphae and arthrospores. Several modifications of the basic 10% KOH preparation have been made for more rapid detection. This includes incorporating Parker super chrome blue in the KOH solution for selective staining of the fungus.
Other modifications of the basic methods include
- Addition of 36% of DMSO to 20% KOH to clearing of the specimen without heating.
- Addition of 5-10% glycerine to the KOH preparation to delay crystallization of the KOH, degrading of the fungus, and dehydration.
- In KOH preparation it is very difficult to differentiate ‘mosaic fungus’ (cholesterol crystals deposited around the periphery of the epidermal cells). It can be recognized by the lack of internal organelles.
- Parker’s ink can also be used for better visualization of Malassezia furfur and (Scopuloropsis spp. and Candida spp.) causing onychomycosis.
KOH with calcofluor white
Calcofluor white is a whitening agent used in the textile and paper industry. A drop of calcofluor white (a fluorescent dye) can be added to the KOH preparation before adding a coverslip. Calcofluor white binds to the polysaccharide present in the chitin or to cellulose. Fungal elements fluoresce apple green or blue-white. So, any element with a polysaccharide skeleton will fluoresce. Although background elements may also fluoresce, the fungal components are brighter.
Culture
Common solid media are as SDA, or DTM with antimicrobial agent and cycloheximide. Small fragments of keratinous material are planted or scattered on SDA containing chloramphenicol and cycloheximide and incubated at room temperature. Growth is slow and colonies may appear in 1-3 weeks. Specialized media may be necessary to stimulate sporulation such as cornmeal agar, potato flake agar, lacrimal rice grains, or PDA so that sporulation will occur. Culture from suspected superficial mycoses is incubated at 30ºC. DTM incorporates gentamicin and chloramphenicol to inhibit the bacteria and a phenol red indicator that changes from yellow to red when the medium becomes alkaline as the result of the growth of dermatophytes.
Identification of culture
Colony characteristics(macroscopy)- Gross colony features observed on SDA include the color of the surface, the color of reverse, texture of the surface(powdery, granular, velvety, or fluffy) type of folding(radial, cerebriform), and the rate of growth.
Microscopic examination of culture
Microscopic characteristics that should be observed are the following:
Septate or aseptate hyphae, hyaline or dematiaceous hyphae, fruiting structures, the types, size, shape, and arrangement of conidia. Microscopic examinations can be studied in teased mounts, slide cultures, or cellophane tape preparation.
Tease mount
With the help of two teasing needles, a portion of the mycelium is removed. An LPCB preparation is prepared on a slide. LPCB does not work well with the dematiaceous fungi because they retain their dark color. The major disadvantage of this procedure is the disruption of conidia during the teasing process. The preparations may be mounted in Poirier’s blue or lactophenol aniline blue or carbol fuchsin.
Cellophane tape preparation
Cellophane tape preparations involve gently touching a piece of clear tape, sticky side down to the surface of the colony, and then removing it. The tape is placed onto a drop of LCB on a slide and examined. With this procedure, the conidial arrangement is retained.
Slide culture
Slide cultures are useful for demonstrating the natural morphology of the fungal structures and for encouraging conidiation in some poorly fruiting fungi. Slide culture is particularly useful when the slide culture from a known isolate is stored in a collection for future comparison against isolates awaiting identification.
Slide culture Technique
Culture character and microscopy of dermatophytes

Physiological and biochemical tests for fungal infections laboratory diagnosis
- Hair perforation test
Trichophyton rubrum, which may be morphologically similar to T. mentagrophytes, usually causes only surface erosion of hair shafts in this test, whereas T. mentagrophytes usually form perpendicular pegs in the hair shafts. This test can also be used to distinguish penetration capable Microsporum canis from M. equinum which does not penetrate the hair. - Urease test
5 days urease test help to differentiate T. mentagrophytes from T. rubrum. Tubes of Christensen urea agar are very lightly inoculated with the dermatophytes and held for 5 days at room temperature. Most isolates of T. mentagrophytes demonstrate urease production resulting in a color change. Most T. rubrum isolates are negative or require more than 5 days to give a positive reaction. - Growth on rice grains
This test is useful to differentiate poorly sporulating isolates of M. canis from M. audouinii. Sterile nonfortified rice is inoculated lightly with a portion of a colony. After 10 days of incubation at room temperature, the medium is observed for growth. M. canis and other dermatophytes grow well and usually form many conidia whereas M. audouinii does not grow but rather turns the rice grains brown.
Subcutaneous mycoses
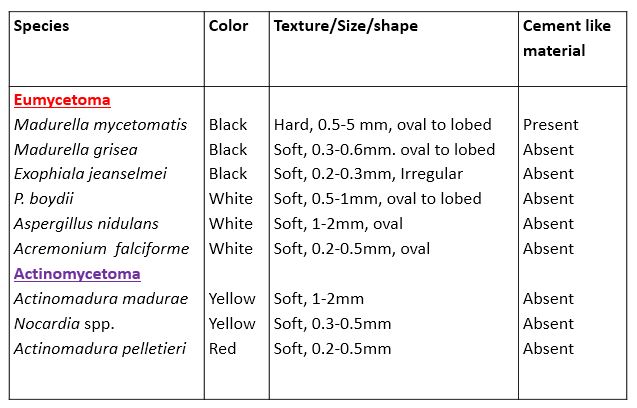
The subcutaneous mycoses comprise a group of fungal infections which are characterized by the development of lesions at the site of implantation of subcutaneous tissues. The disease usually sets in from a trauma which is the sole source of infection. Mycetoma is a unique clinical entity caused by multiple organisms from fungal as well as bacterial origin.
Sample collection from subcutaneous mycoses
The scrapings or crusts from the superficial parts of subcutaneous lesions may be satisfactory. The aspirated samples of pus and biopsy samples are more valuable. The sample of the grains with a deep biopsy is considered best as it contains live granules. In the case of mycetoma, the unruptured pustule is identified, cleaned with an alcohol swab, and gently pierced with a sterile needle.
Processing of specimen fungal infections laboratory diagnosis
The pus containing granules are washed several times with sterile saline in a sterile test tube. After few minutes the granules sediment and these are withdrawn by capillary pipette. The tissue materials are processed for H & E stain. The sputum is first treated with a mucolytic agent and then centrifuged to obtain the granules.
Direct examination
Macroscopy-
The color, shape, size, and texture are noted.
Microscopy
KOH and LCB mount
In the case of mycetoma, the grains in a drop of KOH are crushed with a coverslip by applying pressure over the coverslip. Actinomycotic granules show thin filaments with coccoid or bacillary forms. Eumycotic granules show 2-6 µm wide hyphae. Sporotrichosis shows small, elongated yeast cells. In the case of chromoblastomycosis, muriform bodies(sclerotic bodies) characteristics of all causative agents can be seen.
Gram’s stain
Gram stain can be prepared from different samples obtained. In the case of actinomycetoma, Gram-positive branching filamentous bacteria embedded in the grain material can be seen. Gram-positive Steroid bodies and Sclerotic bodies in cases of sporotrichosis and chromoblastomycosis respectively may be seen. Modified ZN-stain with 1% decolorizer shows pink-colored filamentous bacteria i.e. Nocardia spp.
Biopsy materials
The biopsy materials are stained with H/E, PAS, Gomori’s methenamine silver, Giemsa, and Fontana Masson stains. Tissue containing mycetoma stained with H & E stain shows pale blue to deep blue dots. Melanin is produced in the cell walls of sclerotic bodies which results in dark brown coloration and can be stained with Fontana-Masson stain. Asteroid bodies in tissues are best stained with H & E stain shows pale blue to deep blue surrounded by an eosinophilic halo. MGG stain shows dark blue, thick chitinous walls of sporangia of Rhinosporidium seeberi.
Macroscopic examination of granules for Fungal Infections Laboratory Diagnosis
Culture
The washed granules and other materials obtained from subcutaneous mycoses are cultured on SDA, BHI agar containing chloramphenicol, and cycloheximide. Plates are incubated at 25ºC and 37ºC. Samples should also be cultured on blood agar for actinomycetes. Rhinosporidium seeberi has not been successfully cultured on artificial media. However, it has been grown successfully in vitro in epithelial carcinoma cell culture lines. Slide culture is useful for demonstrating natural morphology.
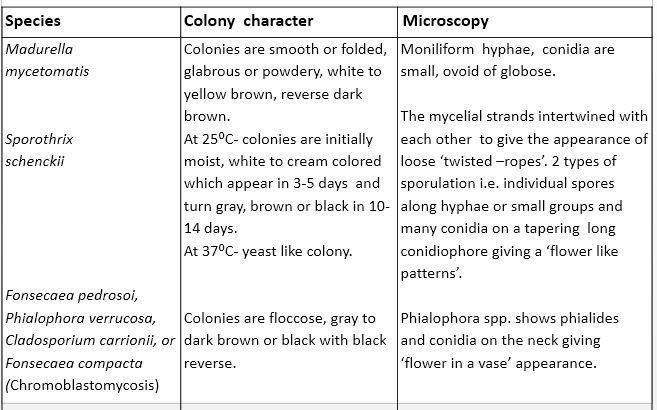
Colony character
Skin test for Fungal Infections Laboratory Diagnosis
The antigen sporotrichin is prepared from the filtrate of 2-3 months mycelial growth in Glucose-yeast extract-casamino liquid medium at room temperature. Intradermal injection of 0.1 ml sporotrichin. More than 5 mm of induration after 48 hours is taken as positive.
Serological tests- The latex particle or whole yeast cell agglutination tests are done for detecting an extracutaneous form of sporotrichosis.
Systemic mycosis
The fungal infections included in this section are mostly caused by dimorphic fungi. All of these diseases were thought to be protozoal at the beginning of their discovery but subsequently identified as fungal in nature. These infections are generally acquired by inhalation of air-born conidia, primarily involving the respiratory system, and are self-limiting and asymptomatic in more than 95% of the patients. In 5% of patients, these are symptomatic and disseminate to other parts of the body through the hematogenous route.
Systemic mycosis is caused by many fungi such as-
Histoplasma capsulatum in tissues develops as narrow-based budding yeast cells. Coccidioides immitis in tissues it develops spherule filled with endospores. Blastomyces dermatitidis in tissues develop broad-based budding yeast cells. Paracoccidioides brasiliensis develops as multiple budding yeast cells.
Sample collection and processing from systemic mycosis for Fungal Infections Laboratory Diagnosis
The specimen includes respiratory secretions, CSF, blood, tissue biopsy, bone marrow, body fluids, and urine.
- Sputum:-The sputum collected for fungal infections should be submitted for 6 successive days. Each day upon awakening in the morning first rinse the mouth and gargle with saline to eliminate the contaminants. Inhale repeatedly to the full capacity of the lungs, exhale the air with an expulsive cough and expectorate in a sterile container.
- Aerosol inhalation (induced sputum):- This procedure is indicated when the patient is not able to produce expectorate. A solution of 150 gm of NaCl dissolved in 200 ml of propylene glycol and mixed with 800 ml of distilled water. This solution is heated to 115 ⁰F and vaporized by means of an air pump. After cleaning the mouth, the patient breaths in and out for 5-10 minutes. The resulting cough-produced sputum is collected in a sterile container.
- Tracheal aspiration:-In this procedure a catheter is moistened in sterile saline and introduced through the mouth or the nares into the trachea of the sitting patient. The secretion is continuously aspirated with a 20 ml syringe
- Bronchial aspiration and washing:- A moistened catheter in sterile saline is introduced into the bronchus. The secretions are aspirated with a syringe. Sterile normal saline is then instilled and allowed to remain in the bronchus for about 5-10 minutes with the patient in a recumbent position. This fluid is aspirated and collected in a sterile container.
- Bronchoalveolar lavage:-In this procedure 100 ml of lukewarm water is used. First washing usually contains most of the contaminants that should be discarded. The subsequent washing is collected in a sterile container.
Processing for Fungal Infections Laboratory Diagnosis
The thick mucoid specimens should be homogenized in an equal volume of N-acetyl L-cysteine. The samples are treated with antibiotics. The material is then centrifuged and the sediment is suspended in 2 ml of sterile saline. The sediment is used for the study. Cycloheximide, an antifungal agent that prevents overgrowth by rapidly growing molds, should be included in at least one of the culture media used.
Cerebrospinal fluid for Fungal Infections Laboratory Diagnosis
CSF collected for culture should be centrifuged and sediment should be used. The media used for the recovery of fungi from CSF should contain no antimicrobial agents because it is a sterile fluid. CSF should be processed immediately. If prompt processing is not feasible, samples should be kept at room temperature.
Blood for Fungal Infections Laboratory Diagnosis
Blood from septicemic patients can harbor both known pathogenic and opportunistic fungi. Blood is collected in a 1:10 ratio of blood to broth in bottles In a smaller set up it may be adequate to use a biphasic brain-heart agar broth. The fungal blood culture media should be incubated at 25 ◦c and 37 ◦c keeping the possibility of any dimorphic fungal agent. They are subcultured after 2 days and 7 days respectively. After subculture, the plates are incubated for 1 week for yeasts and 4-6 weeks for molds. There are several automated blood cultures systems are available like BACTEC and ESP systems for the recovery of fungi. If a high incidence of dimorphic fungi is recovered from blood, the lysis centrifugation system (Isolator) may be used. Using this system RBCs and WBCs which may contain the microorganisms, are lysed and centrifugation concentrates the organisms before culturing. With an Isolator, the cultures are incubated for 3 weeks. The preliminary report is sent after 7 days and the final report after 28 days of the subculture.
Urine for Fungal Infections Laboratory Diagnosis
Urine samples collected for fungal culture should be processed as soon as possible after collection. If delay in culture may be kept at 4◦c for a maximum of 12 hours. All urine samples should be centrifuged and the sediment is cultured using a loop. Because urine is often contaminated with Gram-negative bacteria, it is necessary to use media containing antibacterial agents.
Tissue, bone marrow, and sterile body fluids for Fungal Infections Laboratory Diagnosis
All tissues should be processed before culturing by mincing or grinding. Large portions of tissues should be cut into smaller pieces. Bone marrow may be placed directly onto the surface of appropriate media. Sterile body fluids should be centrifuged and sediment is used for culturing.
Swabs for Fungal Infections Laboratory Diagnosis
Swabs should be heavily charged with exudates, pus, or other secretions. Where plaques are present such as in the mouth, throat(in oral thrush), and vagina(vaginal thrush). The swab should be repeatedly rubbed firmly over these areas. The survival of yeasts on the dry swabs is inversely related to time and storage temperature. If delay can be stored at 4 ◦c and preferably in a suitable transport medium containing antibiotics such as Trichomonas medium.
Stool for Fungal Infections Laboratory Diagnosis
The diagnosis of many fungal infections of the GI tract is better established by biopsy than by the culture of stool samples. Positive culture may be misleading because approximately 40% of healthy individuals and up to 75% of immunocompromised patients are supposed to be colonized with yeasts as commensal.
Eye sample for Fungal Infections Laboratory Diagnosis
In the case of keratomycosis, the corneal scrapings are taken from the margins and base of the ulcer. Using Kimura’s spatula under 4% xylocaine as a local anesthetic.
Laboratory diagnosis of Fungal Infections
Direct examination- KOH and calcofluor white preparation
In the case of Histoplasmosis tiny yeast cells can be seen. In the case of Blastomycosis, double contoured, thick-walled, giant yeast cells with broad-based budding can be seen. In the case of coccidioidomycosis double-refractile, thick-walled globular spherules of 30-60µm in diameter can be seen. In the case of paracoccidioidomycosis round, refractile yeast cells with multiple budding can be seen.
Staining for Fungal Infections Laboratory Diagnosis
The different specimens and histopathological specimens can be stained to reveal the organisms. For staining purposes, Giemsa, PAS, Gomori’s methenamine silver, H&E stains can be used. In the case of histoplasmosis, Giemsa stain shows the cell wall as light blue and dark blue protoplasm. In the PAS stain, the cell wall is red to pink with paler protoplasm filling the cells. In H & E staining the nuclei look deep blue.
Culture for Fungal Infections Laboratory Diagnosis
For culture SDA, BHI agar, blood-glucose cysteine agar, blood agar with antibiotics, and actidione can be used for recovery of fungus. The culture plate is incubated at 25⁰C and 37⁰C for the recovery of mold form as well as yeast form. The classic means for identification is in vitro conversion of dimorphic fungus from yeast to mold form(M Y) and vice versa. Mold to yeast conversion is carried out on blood-glucose cysteine agar, blood agar, cottonseed conversion agar, or BHI agar.
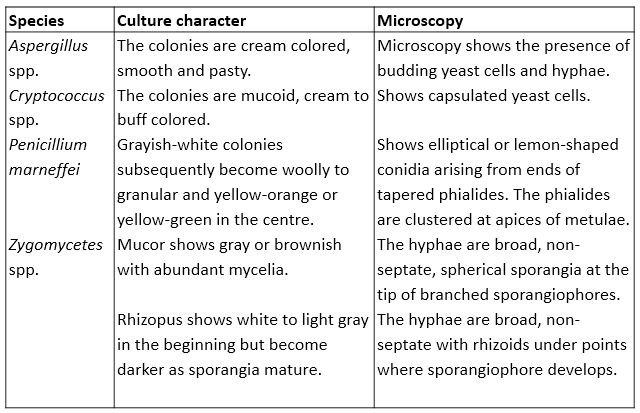
Colony character and microscopy

Slide culture should not be prepared with isolates suspected to be Blastomyces spp., Coccidioides spp., Histoplasma spp. and Paracoccidioides spp. as the risk of infection is too high.
Immunodiagnosis for fungal infections
For immunodiagnosis, 2 types of antigens are used-1. Sterile culture filtrate of broth in which mycelial form has been grown for a period of 3-6 months. 2. A suspension of an inactivated yeast phase.
- Serological tests- Serological test is carried out for the detection of – Specific antibodies and – Circulating antigens. Detection of specific antibody- To detect serum antibodies immunodiffusion, latex agglutination, ELISA, and complement fixation tests are commonly used. Detection of antigen- The serological tests for the detection of antigen using a monoclonal antibody, in body fluids particularly serum may be used especially in immunosuppressed individuals.
- Skin test: The intradermal injection of 0.1 ml of antigen gives an induration of 5 mm or more after 24- 48 hours in a positive case. A positive test shows past or present infection but does not differentiate between them.
Nucleic acid probe for Fungal Infections Laboratory Diagnosis
Genetic probes are available for the detection of Blastomyces dermatitidis, Coccidioides immitis, Cryptococcus neoformans, and Histoplasma capsulatum and other fungi. Detection of fungal DNA by polymerase chain reaction.
Opportunistic mycoses
The opportunistic mycoses are those fungal infections caused by relatively lesser pathogenic, contaminant fungi or commensal fungi in a host whose immunological defense mechanisms are weakened by cancer, leukemia, AIDS, or immunosuppressive therapy. Candida spp, Cryptococcus spp, Penicillium spp, Aspergillus spp, Zygomycetes, etc. are the main fungi causing opportunistic infection.
Sample collection for Fungal Infections Laboratory Diagnosis
The specimen includes respiratory tract secretions, CSF, blood, tissue, bone marrow, body fluids, urine, swab, and stool. Swabs should be heavily charged with exudates, pus, or other secretions. Where plaques are present such as in the mouth, throat(in oral thrush), and vagina(vaginal thrush). The swab should be repeatedly rubbed firmly over these areas. The survival of yeasts on the dry swabs is inversely related to time and storage temperature. Skin and nails can be collected by scraping the affected area,
Processing of specimens for Fungal Infections Laboratory Diagnosis
Specimens are processed for systemic mycoses. A portion of tissue suspected to contain zygomycetes should be finely minced with a pair of scissors or scalpels. It is not recommended to homogenize tissue materials and specimens suspected to contain zygomycetes.
Direct examination for Fungal Infections Laboratory Diagnosis
KOH preparation, calcofluor white preparation can be prepared with the specimens. LCB or Parker’s ink(in mucocutaneous candidiasis) can also be used for direct observation. Budding yeast cells, pseudohyphae, and hyphae in case of candidiasis. In the case of cryptococcosis, budding yeast cells can be seen. Aspergillus shows hyaline, septate hyphae with dichotomous branching.
Zygomycetes show non-septate, ribbon-like hyphae with right-angle branching at irregular intervals. Fixed mounts can be stained with Gram’s stain, methylene blue, H&E stain, or Giemsa stain. Gram staining shows gram-positive budding yeast cells of Candida spp. and Cryptococcus spp. Alcian-blue and mucicarmine staining of histopathological sections are used to demonstrate the capsule. Masson-Fontana stain shows the production of melanin by yeasts hence it is highly significant for detecting capsule deficient cryptococci in tissues. Penicillium marneffei can be seen as basophilic yeast-like cells.
India ink preparation (negative staining) for Fungal Infections Laboratory Diagnosis
India ink preparation may be used to examine CSF for the presence of the encapsulated yeast such as Cryptococcus neoformans. With negative stain, budding yeast surrounded by a large clear area against a black background is presumptive evidence of C. neoformans.
Culture
The routine medium used for the isolation of fungi is SDA supplemented with antibiotics to prevent bacterial growth. Cycloheximide should not be used for suspected specimens having Cryptococcus spp, Aspergillus spp. because these fungi are susceptible to these antibiotics. In Candida spp and Aspergillus spp. the growth appears within 2-3 days therefore cultures should be examined daily for one week and twice a week for the subsequent period.
Serological tests for Fungal Infections Laboratory Diagnosis
Serological tests include the detection of antibodies in serum and specific antigens in the organisms (fungus). Detection by various Ag-Ab reactions eg. agglutination, precipitation, complement fixation, ELISA, and PCR. Antisera reacting against cell wall antigens (cell wall mannoprotein and heat-labile antigen) are commercially available for a number of Candida spp and Cryptococcus neoformans. Candida-specific mannans antigens and Cryptococcus neoformans polysaccharides are detected by antisera.
Detecting Aspergillus-specific galactomannan or glucan by ELISA inpatient sample has demonstrated high sensitivity and specificity. Normal individuals have glucan concentrations less than 10 pg/ml, whereas concentrations more than 20 pg/ml correlates with fungal infections other than zygomycetes. A latex agglutination test is done for cryptococcal antigens in CSF and serum. Another antigen understudy for diagnostic testing is β-(1,3)-D-glucan, a major fungal cell wall constituent. It is observed that deep mycoses including aspergillosis and candidiasis are associated with high plasma levels of this antigen, which is very low in normal serum.
G- test: The recently developed which detects circulating β-(1,3)-D-glucan.
Antigen detection: The serological tests for the detection of antibodies are of limited value in the early stages of infection, in immunocompromised patients, or where the immune response is not sufficient to raise the significant level of antibodies. The diagnosis of cryptococcosis using latex particle agglutination tests for the detection of capsular antigen in CSF and other body fluids. Latex particle agglutination can also be used in aspergillosis and candidiasis.
Skin test
Skin testing is used in the diagnosis of fungal allergies and infections. The sensitization can be shown by skin tests in which induration and erythema occur 2-3 days following intradermal inoculation of the appropriate fungal antigen. Aspergillus antigen extract is used for suspected allergic bronchopulmonary aspergillosis, atopic dermatitis, or allergic asthma. A positive reaction is more likely to suggest a previous infection rather than a current infection
Other tests for the identification of yeasts
Germ tube production test for Fungal Infections Laboratory Diagnosis
Both Candida albicans and C. dubliniensis are germ tube positive. The procedure requires the use of serum or plasma such as fetal bovine serum. Expired fresh frozen plasma can be used. Many other liquid media such as BHI, trypticase soy broth, or nutrient broth can be used as alternative media. The media is inoculated with one yeast colony and incubated at 35 ºC for 2.5-3 hours. Beyond 3 hrs other species are capable of forming germ tubes, so should not be incubated beyond 3 hrs. True germ tubes without constriction at their bases identify C. albicans or C. dubliniensis. If the constriction is present, it is called pseudo germ tubes, which are more characteristic of C. tropicalis. C. albicans is differentiated from C. dubliniensis by its ability to grow at 42-45 ºC and C. dubliniensis is not able to grow at this temperature.
Carbohydrate assimilation test
Carbon assimilation tests identify which carbohydrates, a yeast can utilize as a sole source of carbon aerobically. Yeast and yeast-like fungi utilize specific carbohydrate substances. Organisms are inoculated onto a carbohydrate-free medium. Carbohydrate-containing filter paper disks are added and utilization is determined by the presence of growth around the disk. Characteristic carbohydrate utilization profiles are used to identify species of yeasts.
Use of CHROM agar for Fungal Infections Laboratory Diagnosis
Principle:- CHROM agar contains enzymatic substrates that are linked to chromogenic compounds. When specific enzymes cleave the substrates, the chromogenic substrates produce color. The different species give different colors. Best suited for C. albicans, C. tropicalis, C. dubliniensis, C. krusei and Trichosporon spp.
C. albicans gives light green color.
C. dubliniensis gives dark-green color.
C. tropicalis gives blue to blue-gray color with a paler pink edge.
C. krusei gives a pink colony with a pale pink to the white edge.
Trichosporon spp. gives blue-green colony
Caffeic acid disc test for Fungal Infections Laboratory Diagnosis
Principle:- Caffeic acid is the substrate for the phenoloxidase enzyme produced only by C. neoformans. This enzymatic reaction produces melanin, which is absorbed by the yeast cell wall, resulting in a brown pigmentation.
Method
A disc containing caffeic acid is inoculated with a loop of colonies. After few minutes the colony is changed to a brown color. This brown discoloration is due to the formation of melanin which is absorbed by the yeast cell wall.
Carbohydrate fermentation test for Fungal Infections Laboratory Diagnosis
Principle:- In this test yeasts are incubated in broths of particular carbohydrates and air bubble production is indicated in Durham’s tube. Air bubbles production indicates fermentation of particular carbohydrates.
C. albicans ferments glucose and maltose and does not ferment sucrose.
C. tropicalis ferments glucose, maltose and sucrose.
Bibliography
- Medical Mycology. Editors: Emmons and Binford, 2nd ed 1970, Publisher Lea and Febiger, Philadelphia.
- Rippon’s JW: Medical Microbiology. The pathogenic fungi and the Pathogenic Actinomycetes. 3rd ed 1988 Publisher WB saunder co, Philadelphia.
- Clinical Microbiology Procedure Handbook Vol. I & II, Chief in editor H.D. Isenberg, Albert Einstein College of Medicine, New York, Publisher ASM (American Society for Microbiology), Washington DC.
- A Text-Book of Medical Mycology. Editor: Jagdish Chander. Publication Mehata, India.
- Practical Laboratory Mycology. Editors: Koneman E.W. and G.D. Roberts, 3rd ed 1985, Publisher Williams and Wilkins, Baltimore.
- Topley & Wilsons Medical Mycology. Editors: M.T. Parker & L.H. Collier, 8th ed 1990, Publisher Edward Arnold publication, London.
- Textbook of Diagnostic Microbiology. Editors: Connie R. Mahon, Donald G. Lehman & George Manuselis, 3rd edition2007, Publisher Elsevier.
- Mackie and Mc Cartney Practical Medical Microbiology. Editors: J.G. Colle, A.G. Fraser, B.P. Marmion, A. Simmous, 4th ed, Publisher Churchill Living Stone, New York, Melborne, Sans Franscisco 1996.
- Bailey & Scott’s Diagnostic Microbiology. Editors: Bettey A. Forbes, Daniel F. Sahm & Alice S. Weissfeld, 12th ed 2007, Publisher Elsevier.