
Cryptosporidium: Introduction, Morphology, Life Cycle, Pathogenecity, Lab Diagnosis and Treatment
Introduction of Cryptosporidium
Cryptosporidium is a coccidian protozoan parasite that has gained much attention in the last 20 years as a clinically important human pathogen. For several decades, it was thought to be a rare, opportunistic animal pathogen. It is a spore-producing parasite found in the intestine of infected people and animals. It causes an infection, Cryptosporidiosis. This infection is of two types- a) intestinal cryptosporidiosis-involves watery diarrhea and respiratory cryptosporidiosis-with or without a persistent cough. Cryptosporidiosis primarily involves watery diarrhea with or without a persistent cough in both immunocompetent and immunodeficient humans.
Morphology of Cryptosporidium
It has three developmental stages: meronts, gamonts, and oocysts. Oocyst is the spore phase that can survive for lengthy periods outside a host and it is the infective stage having a size of 4 to 6 μm.
Life Cycle of Cryptosporidium
Excystation of the orally ingested oocyst in the small bowel with the release of the four sporozoites. Invasion of intestinal epithelial cells occurs through the differentiated apical end of the sporozoite within a vacuole. It forms both host and parasite membranes and the initiation of the asexual intracellular multiplication stage happens. Differentiation of microgamete and macrogamete causes fertilization initiating sexual replication. Development of oocysts occurs and the formation of new, infectious sporozoites within the oocyst, which then excretes in the stool.
Mode of infection
Cryptosporidium contaminated food, drinking water, and having close contact with other infected persons are the mode of transmission of this infection.
Pathogenicity of Cryptosporidium
Cryptosporidium is capable of completing its lifecycle within a single host. Oocyst stage that excretes in feces or through inhalation of coughed on fomites and are capable of transmission to a new host. According to report, 8 species of Cryptosporidium infects human and they are C. hominis, C. parvum, C. meleagridis, C. felis, C. canis,C. muris, and C.suis, and the Cryptosporidium cervine genotypes. Cryptosporidium parvum is the most common infecting species. Cryptosporidiosis is typically an acute, short-term infection, can be recurrent through reinfection in immunocompetent hosts, and become severe or life-threatening in immunocompromised individuals. In humans, it remains in the lower intestine and may remain for up to five weeks.
Risk factors
Those who are exposed to contaminated water
Children, particularly those in diapers, who attend child care centers
Parents of infected children
Child care workers
Animal handlers
Those who engage in oral-to-anal sexual activity
International travelers, especially those traveling to developing countries
Backpackers, hikers, and campers who drink untreated, unfiltered water
Swimmers who swallow water in pools, lakes, and rivers
People who drink water from shallow, unprotected wells
Manifestation in Immunocompetent patients
Frequent, watery diarrhea
Nausea
Vomiting
Abdominal cramps
Low-grade fever
In immunocompromised persons
Debilitating, cholera-like diarrhea (up to 20 liters/day)
Severe abdominal cramps
Malaise
Low-grade fever
Weight loss
Laboratory Diagnosis
Acid-fast staining methods, with or without stool concentration, are the most common method for laboratory diagnosis in clinical laboratories. For the greatest sensitivity and specificity, immunofluorescence microscopy is the method of choice. Molecular methods are mainly a research tool. Processing of Stool specimens: submission of stool specimens may be fresh, preserved in 10% buffered formalin, or suspended in a storage medium composed of aqueous potassium dichromate (2.5% w/v, final concentration). Multiple stool samples tests are mandatory before to say the final result is negative.
To maximize recovery of oocysts, concentrate stool samples prior to microscopic examination. Oocyst concentration techniques: Perform Sedimentation methods at low-speed centrifugation. Due to small size and mass, Cryptosporidium oocysts may trap in the ether or ethyl acetate plug and fail to sediment properly. Increased centrifugation speed or time (500 × g, 10 minutes) may warrant when attempting to recover cryptosporidium oocysts. Modified Kinyoun’s Acid-Fast Stain (cold):
Smear 1 to 2 drops of the specimen on the slide, and allow it to air dry. Do not make the smears too thick (you should be able to see through the wet material before it dries). Prepare two smears. Fix with absolute methanol for 1 min.
Flood slide with Kinyoun’s carbol fuchsin, and stain for 5 min. Rinse slide briefly (3 to 5 s) with 50% ethanol. Rinse thoroughly with water. Decolorize with 1% sulphuric acid for 2 min or until no more color runs from the slide.
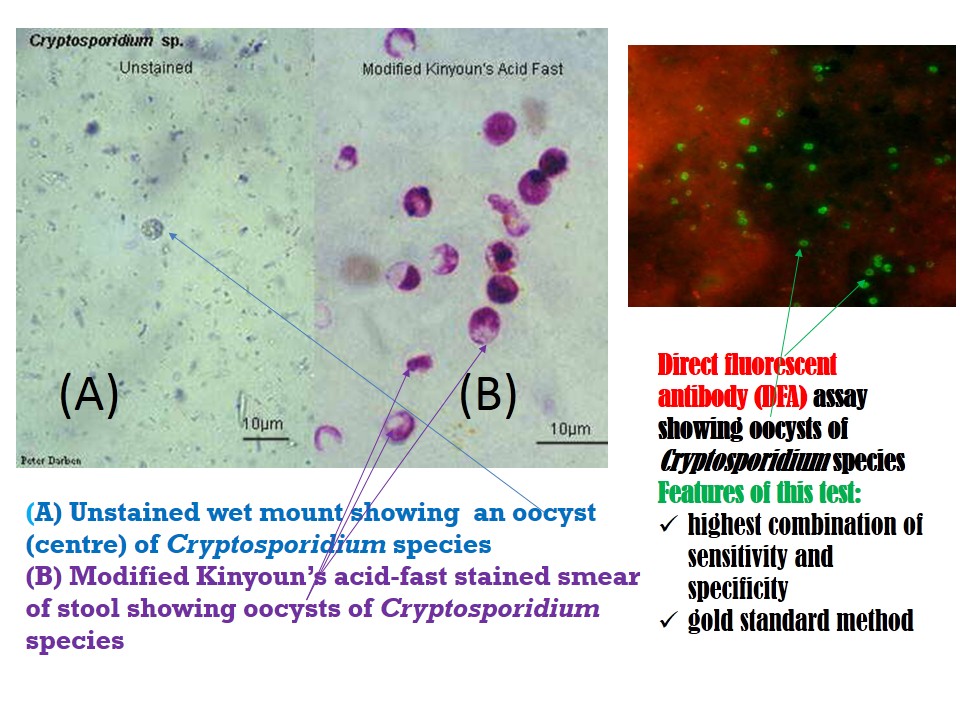
Rinse slide with water. Drain. Counterstain with methylene blue or brilliant green for 1 min. Rinse slide with water. Air dry. Examine using low or high dry objectives. To see internal morphology, use the oil immersion objective (100X). This modified Kinyoun’s Acid-fast staining is a sensitive test. Modified acid-fast stain shows oocysts (4 to 6 μm) often have distinct oocyst walls and stain from light pink to bright red. However, staining may be variable. In particular, infections that are resolving can have colorless oocyst “ghosts.”
Mature oocysts may have discernible sporozoites. Direct fluorescent antibody (DFA) assay: This technique offers the highest combination of sensitivity and specificity and thus considers the gold standard.
Other methods for detecting Cryptosporidium in stool: Enzyme immunoassay (EIA): It is highly sensitive and specific, and is useful for screening large numbers of specimens. Rapid immunochromatographic cartridge assays: It is also helpful with preserved specimens and is quick and easy to perform.Genetic methods in Diagnosis: Genetic methods for detecting oocysts uses that identify and amplify Cryptosporidium nucleic acids using the Polymerase Chain Reaction (PCR).
Treatment of Cryptosporidium
Oral rehydration is a minimal essential treatment
Since cryptosporidiosis is a self-limiting illness in immunocompetent individuals, general, supportive care is the only treatment for the illness.
Oral or intravenous rehydration and replacement of electrolytes may be necessary for particularly voluminous, watery diarrhea. Cryptosporidium treatment options include: Anti-parasitic drugs: Medications such as nitazoxanide (Alinia-Brand name) can help alleviate diarrhea by attacking the metabolic processes of the Cryptosporidium organisms.
Azithromycin along with one of these medications is applicable in people with compromised immune systems. Treatment in Immunosuppressed: The effectiveness of nitazoxanide in Immunosuppressed persons is unclear.
For persons with AIDS, anti-retroviral therapy, which improves immune status, will also reduce oocyst excretion and decrease diarrhea associated with cryptosporidiosis.
Prevention and control
Water
Do not drink contaminated water from the sources like
untreated lakes, rivers, shallow wells.
Treat potentially contaminated water
Heat (rolling boil for one minute)
Filter (absolute pore size of one micron
Food
Wash raw fruits and vegetables
Practice good hygiene
Hand washing
Don’t swim in recreational waters for at least two weeks after symptoms end
Avoid fecal exposure
Limit environmental contamination
Clean and promptly remove feces from surface
Further Readings
- Isenberg clinical microbiology procedures Handbook
2nd edition. Vol. 2 - Merkell and Voge’s medical parasitology
9th edition. - Parasitology: 12th edition
By K. D. Chatterjee - District laboratory practice in Tropical countries –Part-I.
By Monica Chesbrough. - Atlas of Medical Helminthology and protozoology -4th edn -P.L. Chiodini, A.H. Moody, D.W. Manser
- Medical Parasitology by Abhay R. Satoskar, Gary L. Simon, Peter J. Hotez and Moriya Tsuji