
Ochroconis gallopava on SDA: Introduction, Morphology, Lab Diagnosis and Treatment
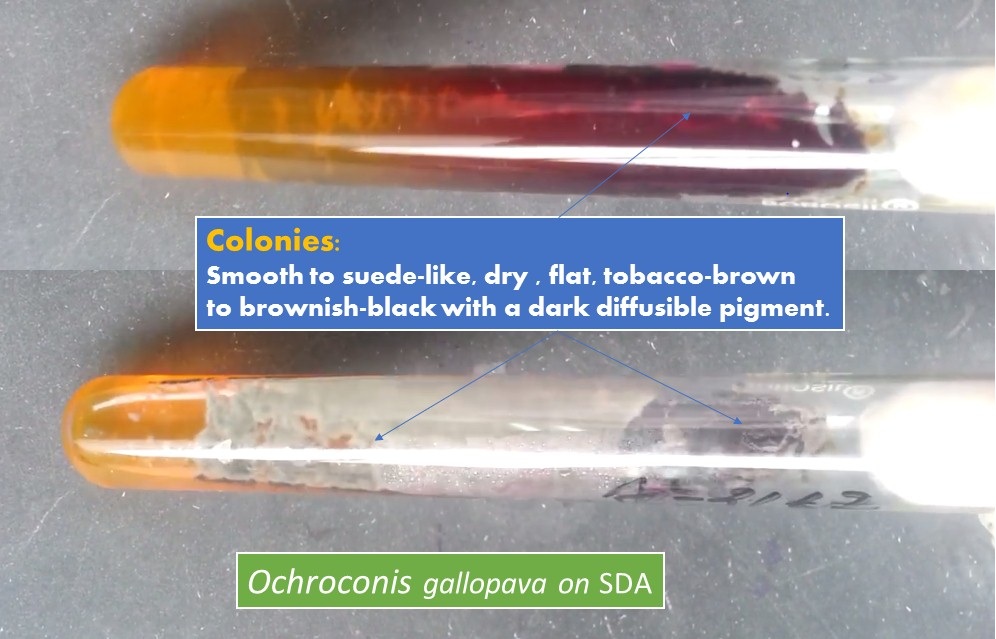
Ochroconis gallopava on SDA
Ochroconis gallopava colonies on SDA are flat, dry and tobacco-brown to brownish-black in color and color due to the principle pigment, melanin and it is distributed throughout the conidia and hyphae. The fungus also releases a dark brown soluble pigment into agar growth media as shown above picture. Ochroconis species are mesophilic saprobes, with an optimum growth temperature between 15 and 30°C and an inability to grow at 37°C whereas maximum growth temperature is around 33°C. It is a thermotolerant, darkly pigmented fungus( dematiaceous ) that causes various infections in immunocompromised hosts. V. gallopava ( Ochroconis transferred to the new genus Verruconis-Samerpitak et al. 2014) was the most common species (69%), followed by O. mirabilis (22%). Other species isolated were O. cordanae, O. olivacea, and O. ramosa. The most common anatomical site of isolation is the lower respiratory tract (59%), followed by superficial (22%) and deep tissues (20%) (Giraldo et al. 2014). The organism has a worldwide distribution, however many cases of human infections have been described in the southeastern USA.
Risk Group: They come in risk group-1 organisms.
Morphology of Ochroconis
Macroscopic characteristics on SDA: Colonies restricted, velvety to funiculose, brown to olivaceous, often with rust-brown reverse. Microscopic properties under the microscope ( LPCB preparation ): Hyphae smooth- or somewhat rough-walled, pale olivaceous. Conidiophores slightly or conspicuously differentiated, cylindrical, often flexuose, producing conidia on scattered, cylindrical to conical denticles. After detachment, an inconspicuous frill often remains both on the denticle and on the conidium base. Conidia one to four-celled, pale olivaceous brown, smooth- or rough-walled, ellipsoidal, cylindrical, clavate, or cuneiform.
Pathogenicity
O. gallopava infection has been very rare, observed in immunologically normal people. Unlike infections in immunocompromised individuals and thus it has been increasingly recognized as a pathogen for humans following solid organ transplantation, such as kidney, liver, heart, and lung. It remains an extremely uncommon agent of human disease. When it does occur in humans, a wide range of sites may become involved, including the lung, heart, brain, superficial cutaneous or subcutaneous areas, and other parts of the body. Like other melanized fungi, the clinical presentation of O. gallopava is phaeohyphomycosis characterized by darkly colored lesions in affected tissues.
Risk factors of this Ochroconis infections
Following are the risk factors of this infection are-
- Hematological malignancies undergoing chemotherapy
- Organ transplantation
- HIV/AIDS and
- Chronic granulomatous disease (CGD)
Symptoms of Ochroconis Infections
Symptoms of this infection depends on the site of involvement such as neurological involvement can show symptoms of migraine, fever, confusion, seizure, lethargy, neck pain, hemiparesis, and paralysis of the legs or both sides of the body whereas respiratory tract infections (RTIs) are associated with milder symptoms such as cough, chest pain, and dyspnea, or maybe entirely asymptomatic. Similarly, other symptoms have been reported including swelling of shoulder and neck and skin granules.
Laboratory Diagnosis
Direct Microscopy: KOH mount-Presence of colored septate hyphae
Culture: Colonies are brown-olive, and have a velvety texture on fungal medium, SDA.
LPCB preparation of culture: In LPCB preparation brown septate hyphae, unbranched conidiophores with apical denticles arranged sympodially, and club-shaped conidia with one to three transverse septa may be seen.
Molecular Identification: Sequencing of ITS and D1/D2 regions of rDNA can be used for molecular identification.
Treatment
Infection treatment widely use antifungal drugs and they are-
- Posaconazole,
- Caspofungin
- Anidulafungin
- Amphotericin b
- Itraconazole
- Terbinafine
- Micafungin
- Voriconazole
Due to the high mortality rate reported in patients (estimated at 50%), proper recognition and treatment of Ochroconis infection are very important. Several studies suggest that posaconazole and itraconazole may be an optimal therapy for this infection, with amphotericin B and voriconazole as valid alternatives. Flucytosine and fluconazole are the least effective drugs. O. gallopava has low MICs for most antifungal drugs with terbinafine, posaconazole, and voriconazole showing the best in vitro activity.
Keynotes
- Giraldo et al. (2014) used sequence analyses of the 18S, ITS, D1/2, actin, and β-tubulin genes, while Seyedmousavi et al. (2014), used ITS sequence analyses to identify species.
- Ochroconis mirabilis, a newly introduced water-borne dematiaceous fungus, is occasionally isolated from human skin lesions and nails and the genomic analysis of this organism UM 578 provides a better understanding of fungal survival tactics in different habitats.
- The lack of knowledge of Ochroconis infections in humans has two potential consequences and they are first, clinicians may fail to consider it in their differential diagnosis while second, the microbiology laboratory may mistakenly dismiss the organism as a contaminant, rather than acknowledging it as a true pathogen.
#Ochroconis gallopava growth on SDA and LPCB preparation as shown below//
References
- https://mycology.adelaide.edu.au/descriptions/hyphomycetes/ochroconis/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4313285/
- https://en.wikipedia.org/wiki/Ochroconis_gallopava
- https://www.sciencedirect.com/science/article/pii/S1198743X14602305
- https://www.researchgate.net/publication/280032657_Three_New_Species_of_the_Genus_Ochroconis
- https://bmcgenomics.biomedcentral.com/articles/10.1186/s12864-016-2409-8