
Rothia kristinae: Introduction, Pathogenicity, Lab Diagnosis, Treatment, Prevention, and Keynotes
Introduction & Taxonomy
Rothia kristinae is a Gram-positive bacterium increasingly recognized as an emerging opportunistic pathogen. While typically a harmless commensal of human skin and mucosal surfaces, it can cause severe systemic infections, particularly in individuals with compromised immune systems or indwelling medical devices.
- Classification: A member of the Micrococcaceae family, this organism was originally classified as Micrococcus kristinae (1974), moved to Kocuria (1995), and finally reclassified as Rothia in 2018 based on genomic data.
- Habitat: It colonizes human skin, the oropharynx, and the upper respiratory tract.
Pathogenicity & Clinical Manifestations
- Risk Factors: Primarily affects immunocompromised patients, such as those with cancer or indwelling devices.
- Clinical Picture: Causes infections, including catheter-related bacteremia (~36% of cases) and endocarditis (~13.7%).
- Virulence: Known to form biofilms on medical devices.
Laboratory Diagnosis of Rothia kristinae
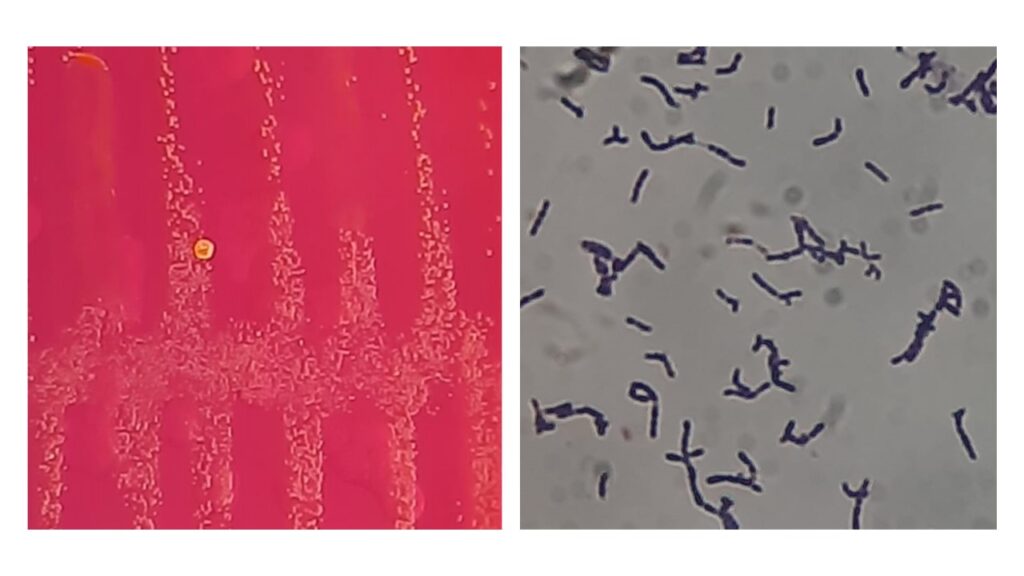
- Identification: Appears as Gram-positive, non-motile cocci in pairs or clusters. Grows on blood agar within 48 hours, forming pale to orange colonies.
- Biochemical Profile: Catalase-positive, but oxidase and coagulase-negative.
- Distinction: Often distinguished from Staphylococcusby susceptibility to bacitracin and resistance to lysostaphin.
- Gold Standard: Identification is best achieved via 16S rRNA sequencing or MALDI-TOF MS.
Treatment & Prevention
- Treatment: Vancomycin is typically effective, along with linezolid or rifampicin, though resistance to certain drugs, such as clindamycin, can occur.
- Management: Successful treatment often requires removing infected catheters.
- Prevention: Adherence to infection control protocols (e.g., CLABSI bundles) is critical.
Keynotes on Rothia kristinae
- R. kristinaes should not be dismissed as a contaminant, particularly in recurring blood cultures.
- Commonly misidentified in labs as Coagulase-Negative Staphylococci (CoNS).
Further Readings
- https://pmc.ncbi.nlm.nih.gov/articles/PMC11991707
- https://medicallabnotes.com/rothia-kristinae-introduction-pathogenicity
- https://www.idcmjournal.org/wp-content/uploads/2025/03/IDCM-2025-436.pdf
- https://www.ovid.com/journals/idcpr/pdf/10.1097/ipc.0000000000001465~rothia-kristinae-nosocomial-sepsis-with-prolonged-bacteremia
- https://pdfs.semanticscholar.org/a5ff/e64b14192cc8215ad5ed850881b5be48e2b5.pdf
- https://en.wikipedia.org/wiki/Rothia_kristinae
- https://en.wikipedia.org/wiki/Rothia_kristinae
- https://revistascientificas.cuc.edu.co/JACN/article/download/6569/5870/57451
- https://www.sciencedirect.com/science/article/abs/pii/S156713482100174X
[207 visitors]