
Pus Cell, Bacteria, and RBC in the Urine of UTI Patient: Introduction, Wet Mount Preparation and Related Videos
Pus Cell, Bacteria, and RBC in Urine of UTI Patient
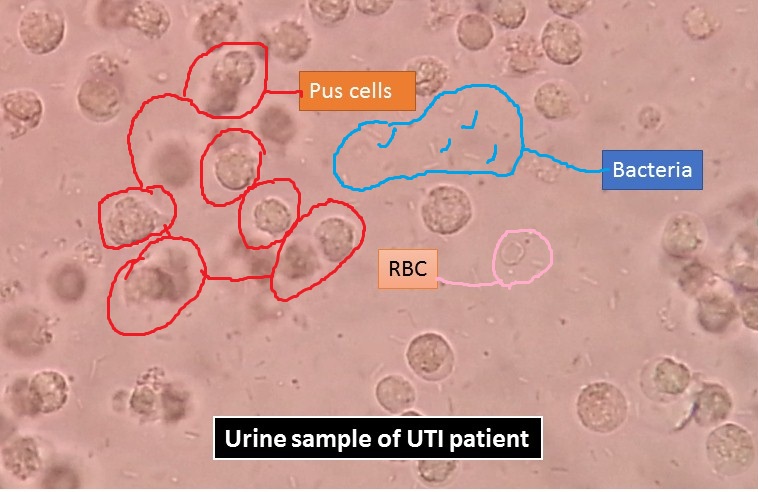
Pus cell, bacteria, and RBC in the urine of UTI patient as shown above picture. Pus is an exudate, typically white-yellow, yellow, or yellow-brown, formed at the site of inflammation during infection (bacterial or fungal ). An abscess is an accumulation of pus in an enclosed tissue space whereas a visible collection of pus within or beneath the epidermis is a pustule, pimple, or spot. Pus consists of a thin, protein-rich fluid and dead leukocytes from the body’s immune response (mostly neutrophils).
Pyogenic ( pus-forming) bacteria
Following common bacteria are responsible for the production of pus and they are-
- Staphylococcus aureus
- Staphylococcus epidermidis
- Streptococcus pyogenes
- Escherichia coli (Bacillus coli communis)
- Streptococcus pneumoniae (Fraenkel’s pneumococcus)
- Klebsiella pneumoniae (Friedländer’s bacillus)
- Salmonella typhi (Bacillus typhosus)
- Pseudomonas aeruginosa
- Neisseria gonorrhoeae
- Actinomyces
- Burkholderia mallei (Glanders bacillus)
- Mycobacterium tuberculosis (tubercle bacillus)
#How to test pus culture and sensitivity a shown below-
Preparation for Microscopic examination of Urine
Requirements
- Specimen ( urine)
- Clean and grease-free slides
- Coverslip
- Microscope
- Centrifuge
- Centrifuge tubes
Test procedure
- Centrifuge a sample of well-mixed urine (usually 10-15 ml) in a test tube at relatively low speed (about 2000-3,000 rpm) for 5-10 minutes which produces a concentration of sediment (cellular matter) at the bottom of the tube.
- Pour a drop of sediment onto a glass slide and then place a thin slice of glass (a coverslip) over it.
- Observe under a microscope.
- Examine the entire 22- by 22-mm coverslip systematically with the low power objective (10X ) and low light intensity.
- If any suspicious objects encounter, examine with the high dry objective (40X).
Clinical significance of Microscopic examination of urine
A variety of normal and abnormal cellular elements may be seen in urine sediment such as-
- Red blood cells
- White blood cells
- Mucus
- Various epithelial cells
- Various crystals
- Bacteria
- Casts
Morphology and Clinical Significance of Pus Cell, Bacteria RBC in Urine of UTI Patient
White Blood Cells (WBCs)
WBCs 12 µm Neutrophil is predominant Identify under high power
WBC in high numbers indicates inflammation or infection somewhere along with the urinary system.
Glitter cells: They are polymorphonuclear cells (neutrophils) that are found in the urine, most commonly associated with urinary tract infections( UTIs) and pyelonephritis. Their name is called so because of their appearance when viewed on a wet mount preparation under a microscope; the granules within their cytoplasm can be seen moving, giving them a “glittering appearance.
Hypotonic urine
Brownian movement
Swell; granules sparkle
Pale blue if stained
Nonpathologic
Eosinophils Hansel stain
Drug-induced interstitial nephritis
Renal transplant rejection
Hansel stain
Percent per 100 to 500 cells
>1% significant
Concentrate sediment, centrifuge, or cytocentrifuge
Mononuclear cells
Lymphocytes, monocytes, macrophages, histiocytes are rare
Differentiate from renal tubular epithelial (RTE) cells
Staining
Lymphocytes may resemble RBCs; seen in early transplant rejection
May need to refer to cytodiagnostic testing
Clinical Significance of WBCs
Normal = <5 per HPF, more in females
May enter through glomerulus or trauma but also by amoeboid migration
Increased WBCs = pyuria
Infections: cystitis, pyelonephritis, prostatitis, urethritis
Glomerulonephritis, lupus erythematosus, interstitial nephritis, tumors
Report presence of bacteria
Bacteria
Urine is usually sterile, contaminated on the way out; contaminants multiply fast in urine and itself a good medium for bacteria.
WBCs should accompany bacteria in UTI
Report few, moderate, many highs per field (HPF)
Rods and cocci may be seen; rods most common
Nitrite helps to confirm rods, not cocci
Red Blood Cells (RBCs)
RBCs Smooth, nonnucleated, biconcave disks nearly 7 µm
Crenated in hypersthenuric urine
Ghost cells in hyposthenuric urine
Dysmorphic RBCs
Glomerular bleeding
Strenuous exercise
Acanthocytic, blebs
Fragmented, hypochromic
Aid in diagnosis
Clinical Significance
Normal value: 0–3 to 5/hpf
Hematuria is the presence of abnormal numbers of red cells in urine due to several possible causes.
Damage to the glomerular membrane of vascular injury to the genitourinary tract
Number of cells = extent of damage
Macroscopic versus microscopic hematuria
Cloudy, red urine, advanced disease, trauma, acute infection, coagulation disorders
Clear urine, early glomerular disease, malignancy, strenuous exercise, renal calculi confirmation
Pus sample under the microscope showing plenty dead white blood cells (pus cells)
Pus cells in stool
Pus cells in sputum
Pus cells in CSF
Pus cells in pleural fluid
Pus cells in vaginal swab
Bibliography
- https://www.healthline.com/health/pus
- https://pmj.bmj.com/content/postgradmedj/43/499/376.full.pdf
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4692015/
- https://anesthesiology.pubs.asahq.org/article.aspx?articleid=1934439
- https://doctor.ndtv.com/faq/what-do-the-levels-of-pus-cells-in-urine-indicate-11172
- https://www.researchgate.net/post/Are_pus_cells_in_CSF_always_associated_with_only_bacterial_meningitis
- https://www.healthgrades.com/right-care/symptoms-and-conditions/pus
- https://www.medicalnewstoday.com/articles/249182
- https://en.wikipedia.org/wiki/Pus
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2018983/pdf/archdisch01591-0064.pdf
- https://slideplayer.com/slide/4888984/
- http://www.journalofdiabetology.org/article.asp?issn=2078-7685;year=2019;volume=10;issue=3;spage=102;epage=109;aulast=Patra
- https://www.kidney.org/atoz/content/what-urinalysishttps://advuro.com/urinary-conditions/pyuria/
- https://adc.bmj.com/content/archdischild/44/236/480.full.pdf
- https://en.wikipedia.org/wiki/Glitter_cell
- https://www.verywellhealth.com/what-is-pyuria-3522705