
Introduction
Morganella is a genus of gram-negative bacteria belonging to the family Enterobacteriaceae. It was named after the bacteriologist Carl Wilhelm Julius Friedrich Julius Morgan, who first described it in 1906. The genus Morganella includes three species: M. morganii, M. psychrotolerans, and M. osloensis.
Among the species in this genus, Morganella morganii is the most clinically relevant and frequently encountered. It is a facultative anaerobe, meaning it can survive in both aerobic (oxygen-rich) and anaerobic (oxygen-depleted) environments. It is widely distributed in nature, including in soil, water, and the intestinal tracts of humans and animals.
In the clinical setting, M. morganii can be an opportunistic pathogen, causing various infections in humans. It is commonly associated with urinary tract infections, particularly in individuals with compromised immune systems or those with urinary tract abnormalities. Other infections caused by M. morganii include pneumonia, bloodstream infections (sepsis), surgical site infections, and wound infections.
M. morganii possesses certain characteristics that contribute to its pathogenicity. It has a motile nature due to the presence of flagella, which enables it to move and colonize different areas of the body. The bacteria also produce various enzymes, including beta-lactamases, which can confer resistance to certain antibiotics.
In terms of treatment, Morganella morganii infections are usually managed with antibiotics, although resistance to commonly used drugs has been observed. The choice of antibiotic therapy depends on the susceptibility of the specific bacterial strain and the site of infection. In severe cases, a combination of antibiotics may be necessary.
It’s important to note that accurate identification of Morganella species is crucial, as other Enterobacteriaceae species may have similar characteristics. Proper identification helps guide appropriate treatment and infection control measures.
Morphology
The morphology of Morganella bacteria, specifically M. morganii, can be described as follows:
- Shape: It is a rod-shaped bacterium, meaning it appears as a straight or slightly curved cylindrical structure. The cells typically have rounded ends.
- Size: The size of M. morganii cells can vary, but they generally measure around 1-2 micrometers in width and 2-5 micrometers in length.
- Gram Staining: It is a gram-negative bacterium. This means that during the Gram staining process, it appears pink or red under a microscope.
- Flagella: It is motile due to the presence of peritrichous flagella. Peritrichous flagella are distributed all over the surface of the bacterial cell, allowing it to move and navigate its environment.
- Capsule: Some strains of M. morganii may produce a slimy capsule surrounding the bacterial cell. The capsule helps protect the bacteria from the host’s immune system and can contribute to its virulence.
- Spore Formation: M. morganii is non-spore-forming. Spore formation is a characteristic observed in certain bacteria as a means of survival under unfavorable conditions.
Pathogenicity
M. morganii, the most clinically significant species within the Morganella genus, can be an opportunistic pathogen in humans. Its pathogenicity refers to its ability to cause various infections, particularly in individuals with compromised immune systems or those with underlying medical conditions. Here are some key aspects of M. morganii’s pathogenicity:
- Infection Sites: It can cause infections in various anatomical sites, including the urinary tract, respiratory tract, bloodstream, surgical sites, and wounds. Urinary tract infections (UTIs) are particularly common, especially in patients with indwelling urinary catheters or urinary tract abnormalities.
- Adhesion and Invasion: It possesses mechanisms to adhere to and invade host tissues. The bacterial cells can adhere to the lining of the urinary tract or respiratory tract, allowing them to establish an infection. Once attached, they can invade the host’s cells and cause damage.
- Virulence Factors: It produces several virulence factors that contribute to its pathogenicity. These include adhesins, which aid in attachment to host cells, and various enzymes such as hemolysins and proteases, which can damage host tissues and help the bacteria evade the immune system. M. morganii can also produce a cytotoxic necrotizing factor, which contributes to tissue damage.
- Antibiotic Resistance: Some strains of Morganella morganii have shown resistance to multiple antibiotics, including beta-lactam antibiotics. This resistance can make treating infections more challenging and may require the use of alternative antibiotics or combination therapy.
- Complications: Infections caused by M. morganii can lead to various complications depending on the site of infection. For example, urinary tract infections can progress to pyelonephritis (kidney infection), and bloodstream infections can result in sepsis, a severe and potentially life-threatening condition.
- Nosocomial Infections: Morganella morganii infections are often associated with healthcare settings, making them an important cause of nosocomial (hospital-acquired) infections. Factors such as the use of invasive medical devices, prolonged hospital stays, and exposure to antibiotics can increase the risk of these infections.
Effective management of Morganella morganii infections involves prompt and accurate diagnosis, appropriate antibiotic therapy based on susceptibility testing, and infection control measures to prevent its spread in healthcare settings.
Lab Diagnosis
The laboratory diagnosis of Morganella, particularly M.morganii, involves several steps to identify and confirm the presence of the bacterium. Here’s an overview of the laboratory procedures commonly used for diagnosis:
- Specimen Collection: The appropriate specimen is collected based on the suspected site of infection. For example, urine samples are collected for suspected urinary tract infections, wound swabs for wound infections, or blood cultures for bloodstream infections.
- Microscopic Examination: A Gram stain of the specimen is performed to visualize the bacterial morphology. It appears as gram-negative rods under the microscope.
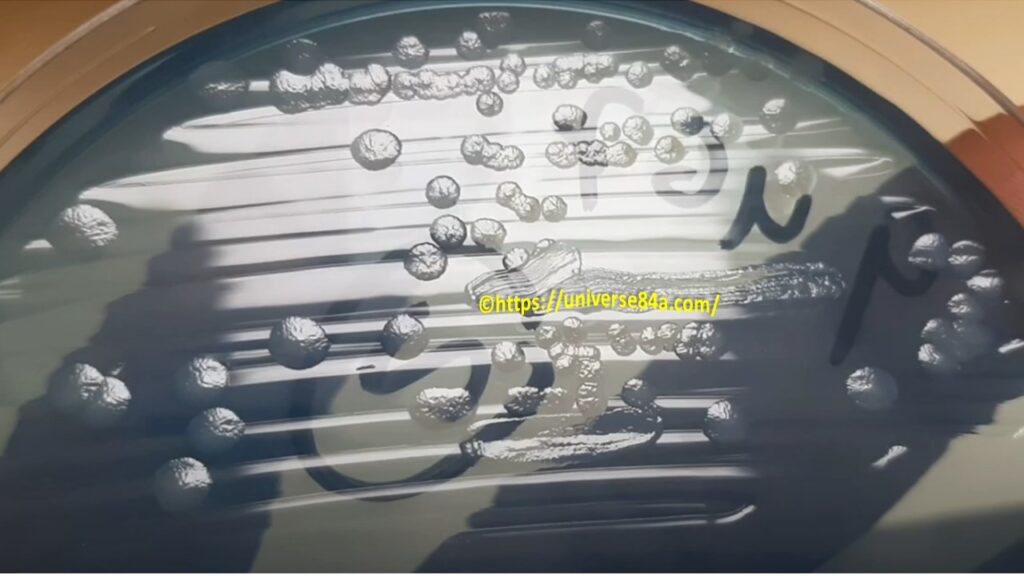
- Culture: The specimen is inoculated onto appropriate culture media, such as blood agar or MacConkey agar, and incubated at the appropriate temperature (usually around 37°C) for bacterial growth. M. morganii typically grows on these media within 24-48 hours.
- Colony Morphology: After incubation, the bacterial colonies are examined for their morphological characteristics. Its colonies on blood agar appear as small to medium-sized, grayish or pale yellow colonies with a characteristic odor. On MacConkey agar, they typically appear as lactose-fermenting colonies, producing pink/red coloration.
- Biochemical Tests: Several biochemical tests are performed to further identify and differentiate M. morganii from other bacteria. These tests may include the catalase test (positive), oxidase test (negative), indole production (positive), urease production (positive), and citrate utilization (negative).
- Antimicrobial Susceptibility Testing: It is essential to determine the susceptibility of the M. morganii isolate to various antibiotics. This is done through antimicrobial susceptibility testing, such as the disk diffusion method or automated systems, following established guidelines. It helps guide appropriate antibiotic treatment.
- Confirmation: To confirm the identification of Morganella morganii, additional tests like DNA sequencing or matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) can be performed. These tests provide accurate and definitive identification of the bacterial species.
Treatment
The treatment of Morganella infections, particularly those caused by Morganella morganii, involves the administration of appropriate antibiotics based on the susceptibility of the bacterial strain. Here are some general considerations for the treatment of Morganella infections:
- Antibiotic Selection: Morganella morganii is known to exhibit resistance to certain antibiotics, including beta-lactam antibiotics. Therefore, it is crucial to perform antimicrobial susceptibility testing to guide antibiotic selection. The choice of antibiotics may vary based on local resistance patterns and individual patient factors.
- Empirical Therapy: In cases where the susceptibility of the Morganella strain is not known, initial treatment is often initiated empirically with broad-spectrum antibiotics that cover a wide range of potential pathogens, including Morganella morganii. Common choices for empirical therapy may include third-generation cephalosporins (e.g., ceftriaxone, ceftazidime), fluoroquinolones (e.g., ciprofloxacin), or carbapenems (e.g., meropenem, imipenem).
- Susceptibility-Guided Therapy: Once the antimicrobial susceptibility results are available, the antibiotic regimen can be adjusted accordingly. The goal is to select the most effective antibiotic with in vitro activity against the specific strain of Morganella morganii. The susceptibility profile will guide the choice of antibiotics, and the regimen may need to be modified accordingly.
- Combination Therapy: In severe or complicated infections, combination therapy with two or more antibiotics may be considered. This approach helps to broaden the spectrum of coverage, improve the efficacy of treatment, and prevent the development of antibiotic resistance. The choice of combination therapy should be based on susceptibility testing and clinical judgment.
- Duration of Therapy: The duration of antibiotic treatment for Morganella infections depends on the site and severity of infection, as well as individual patient factors. In uncomplicated urinary tract infections, a shorter course of antibiotics (e.g., 7-10 days) may be sufficient. However, in more serious infections or those involving other sites, longer treatment durations (e.g., 10-14 days or more) may be required.
- Follow-Up and Monitoring: Close monitoring of the patient’s clinical response to treatment is essential. It is important to assess for signs of improvement and resolution of infection. If there is no clinical improvement or worsening of symptoms, reevaluation of the antibiotic regimen may be necessary, considering factors such as antibiotic resistance, proper dosing, and source control if applicable.
It’s important to note that treatment should be individualized based on factors such as the specific site of infection, the severity of illness, patient factors (e.g., immune status, allergies), and antimicrobial susceptibility patterns. Therefore, it is advisable to consult with a healthcare professional for a proper evaluation and guidance regarding the treatment of Morganella infections.
Prevention
Preventing Morganella infections involves implementing strategies to reduce the risk of exposure and transmission of the bacteria. Here are some preventive measures that can help minimize the incidence of Morganella infections:
- Infection Control in Healthcare Settings: Adhering to strict infection control practices in healthcare facilities is crucial to prevent the spread of Morganella and other healthcare-associated infections. This includes proper hand hygiene, appropriate use of personal protective equipment, adherence to aseptic techniques during invasive procedures, and proper disinfection and sterilization of medical equipment.
- Catheter Care: Urinary catheters are a common risk factor for urinary tract infections caused by Morganella morganii. To reduce the risk of infection, catheters should be used only when necessary, and their duration of use should be minimized. Proper catheter insertion technique, catheter care, and regular catheter maintenance are essential to prevent bacterial colonization and infection.
- Antimicrobial Stewardship: Implementing antimicrobial stewardship programs in healthcare facilities can help prevent the development of antibiotic resistance. These programs promote the appropriate and judicious use of antibiotics, including correct dosing, duration, and selection of antibiotics based on susceptibility testing.
- Environmental Hygiene: Ensuring cleanliness and proper disinfection of the environment, particularly in healthcare facilities, can help reduce the reservoir and transmission of Morganella morganii. Regular cleaning and disinfection of surfaces and equipment using appropriate disinfectants can help prevent the spread of bacteria.
- Education and Awareness: Healthcare providers and patients should be educated about the risks of Morganella infections and preventive measures. This includes proper hand hygiene, adherence to infection control practices, and recognizing the signs and symptoms of infection to seek timely medical attention.
- Personal Hygiene: Individuals should maintain good personal hygiene practices, including regular handwashing with soap and water or using alcohol-based hand sanitizers. Proper hygiene can help prevent the transmission of bacteria from contaminated surfaces or through person-to-person contact.
It’s important to note that these preventive measures are not specific to Morganella alone but are general infection prevention strategies. Adhering to these practices can help minimize the risk of various healthcare-associated and community-acquired infections, including those caused by Morganella morganii.
Keynotes
Sure! Here are some key points to remember about Morganella:
- Genus: Morganella is a genus of gram-negative bacteria belonging to the family Enterobacteriaceae.
- Species: The most clinically relevant species within the genus is Morganella morganii, although there are other species like Morganella psychrotolerans and Morganella osloensis.
- Morphology: Morganella morganii appears as rod-shaped (bacillus) bacteria with rounded ends. It is gram-negative, motile (with peritrichous flagella), and typically lacks a capsule.
- Pathogenicity: Morganella morganii is an opportunistic pathogen that can cause various infections in humans, including urinary tract infections, respiratory tract infections, bloodstream infections, surgical site infections, and wound infections.
- Virulence Factors: Morganella morganii produces virulence factors such as adhesins, hemolysins, proteases, and cytotoxic necrotizing factors, which contribute to its ability to colonize and invade host tissues.
- Antibiotic Resistance: Some strains of Morganella morganii may exhibit resistance to certain antibiotics, including beta-lactam antibiotics. Antimicrobial susceptibility testing is necessary to guide appropriate antibiotic therapy.
- Nosocomial Infections: Morganella morganii infections are often associated with healthcare settings and can be a cause of nosocomial (hospital-acquired) infections, particularly in patients with indwelling medical devices or prolonged hospital stays.
- Laboratory Diagnosis: The diagnosis of Morganella involves specimen collection, microscopic examination, culture, biochemical tests, and confirmation through additional tests like DNA sequencing or MALDI-TOF MS.
- Treatment: Treatment of Morganella infections involves appropriate antibiotic therapy based on susceptibility testing. Empirical therapy may be initiated initially, followed by adjustment based on susceptibility results. Combination therapy and the duration of treatment may be considered based on the severity and site of infection.
- Prevention: Preventive measures for Morganella infections include strict infection control practices in healthcare settings, catheter care, antimicrobial stewardship, environmental hygiene, education, and personal hygiene.
Further Readings
- Tumbarello M, Spanu T, Sanguinetti M, Citton R, Montuori E, Leone F, Fadda G, Cauda R. 2006. Bloodstream infections caused by extended-spectrum-beta-lactamase-producing Escherichia coli: risk factors for inadequate initial antimicrobial therapy. Antimicrobial Agents and Chemotherapy, 50(9), 3171-3179.
- Yoh M, Matsuyama J, Ohnishi M, Takagi K, Miyagi H, Mori K, Park KS, Ono T, Honda T. 2005. Importance of Providencia species as a major cause of travellers’ diarrhoea. Journal of Medical Microbiology, 54(11), 1077-1082.
- Bergmans DC, Bonten MJ, Stobberingh EE, van Tiel FH, van der Geest S, De Leeuw PW, Stobberingh EE. 1997. Epidemiology of nosocomial infections caused by methicillin-resistant Staphylococcus aureus in The Netherlands, 1992-1996. Clinical Infectious Diseases, 24(4), 684-694.
- Kim BN, Kim NJ, Kim MN, Kim YS, Woo JH, Ryu J, Kim YS. 2001. Bacteremia due to Morganella morganii: clinical significance of the AmpC beta-lactamase production in Morganella species. Journal of Korean Medical Science, 16(6), 791-795.
- Centers for Disease Control and Prevention (CDC). Healthcare-associated Infections (HAI). Available at: https://www.cdc.gov/hai/index.html
- European Centre for Disease Prevention and Control (ECDC). Antimicrobial Resistance Surveillance in Europe. Available at: https://www.ecdc.europa.eu/en/antimicrobial-resistance/surveillance-and-disease-data/data-ecdc