

Kingella kingae case report
Patient history
A patient, 69 years old male having diabetes mellitus past 10 years since two years in insulin. Having a history of mild fever, cough, chest pain with sputum and also throat itching took part in ENT-OPD and the doctor suggested for chest X-ray and sputum culture and sensitivity and requested to follow up after three days with reports.
Kingella, which belongs to the family Neisseriaceae, is short, nonmotile, oxidase-positive but catalase-negative gram-negative coccobacilli, that occur in pairs or short chains. The organism is slow-growing and fastidious. Beta hemolytic colony on 5% sheep blood agar. It is recovered from the human respiratory tract and is a rare cause of human disease. Among Kingella species, K. kingae is the most frequent human pathogen. It frequently colonizes the respiratory mucous membranes. Children with 4-6 years of age have the highest rates of colonization and invasive disease from this respiratory tract pathogen. K. kingae is transmitted from child to child through close personal contact.
Pathogenicity
Kingella comes in the HACEK group and this group contains Haemophilus (species aphrophilus and parainfluenzae), Aggregatibacter, Cardiobacterium, Eikenella, and Kingella), that includes fastidious gram-negative bacteria capable of causing endocarditis. Kingella also causes skeletal infections and bacteremia and, rarely pneumonia, epiglottitis, abscesses, meningitis, and ocular infections.
Lab Diagnosis
X-ray report: Normal
Sputum C/S: Kingella kingae isolates
Sensitivity: Sensitive- Ciprofloxacin
Amoxycillin
Ceftriaxone
Amikacin
Amoxycillin clavulanic acid
Resistant- Co-trimoxazole
Kingella kingae supporting features:
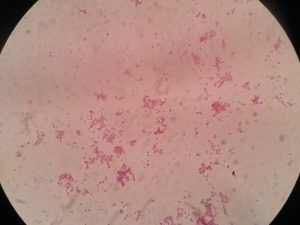
Gram stain finding–
pus cell plenty ( pus cells>25 LPF, epithelial cells<10LPF)
Gram-negative rods with square ends, lying in pairs and also in chains.
Growth on blood agar–
Beta-hemolytic colonies
Biochemical tests–
Catalase- Negative
Oxidase- Positive
Nitrate to nitrite reduction-Negative
Maltose acid- Positive
Photos:







Treatment
Finally patient benefited after oral medication of Ciprofloxacin. Penicillin and cephalosporin are useful to treat even though antimicrobial sensitivity testing is necessary to provide a selective drug of choice. Recommended drugs are aminoglycosides, tetracycline, fluoroquinolones, erythromycin, and trimethoprim-sulfamethoxazole.

Bibliography
- Cowan & Steel’s Manual for identification of Medical Bacteria. Editors: G.I. Barron & R.K. Felthani, 3rd ed 1993, Publisher Cambridge University press.
- Bailey & Scott’s Diagnostic Microbiology. Editors: Bettey A. Forbes, Daniel F. Sahm & Alice S. Weissfeld, 12th ed 2007, Publisher Elsevier.
- Clinical Microbiology Procedure Hand book Vol. I & II, Chief in editor H.D. Isenberg, Albert Einstein College of Medicine, New York, Publisher ASM (American Society for Microbiology), Washington DC.
- Colour Atlas and Text book of Diagnostic Microbiology. Editors: Koneman E.W., Allen D.D., Dowell V.R. Jr and Sommers H.M.
- Jawetz, Melnick and Adelberg’s Medical Microbiology. Editors: Geo. F. Brook, Janet S. Butel & Stephen A. Morse, 21st ed 1998, Publisher Appleton & Lance, Co Stamford Connecticut.
- Mackie and Mc Cartney Practical Medical Microbiology. Editors: J.G. Colle, A.G. Fraser, B.P. Marmion, A. Simmous, 4th ed, Publisher Churchill Living Stone, New York, Melborne, Sans Franscisco 1996.
- Text book of Diagnostic Microbiology. Editors: Connie R. Mahon, Donald G. Lehman & George Manuselis, 3rd edition2007, Publisher Elsevier.