
Entamoeba histolytica Trophozoite in Saline Preparation of Stool and Details About This Parasite
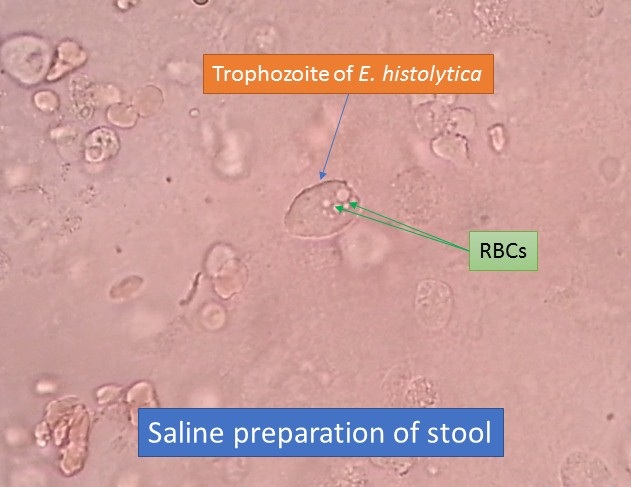
Trophozoite of Entamoeba histolytica in Saline Preparation of Stool
Trophozoite of Entamoeba histolytica in saline preparation of stool as shown above image. Trophozoite has the following features-
- It is the growing or feeding stage.
- The only form is present in the tissue.
- It usually appears only in diarrheic feces and survives only for few hours.
- It exhibits slow gliding movement with pseudopodium and having a shape is not fixed due to constantly changing position.
- Its size is 10-60μm (20-30μm average).
Introduction of Entamoeba histolytica
Entamoeba histolytica is an invasive enteric protozoan parasite that is the cause of amebiasis. It derives its name from its ability to lyse virtually every tissue in the human body and in the bodies of experimental animals.
Habitat of Entamoeba histolytica
Trophozoites of Entamoeba histolytica resides in the mucosa and submucosa of the large intestine of man.
Morphology of Entamoeba histolytica
Entamoeba histolytica exists in 3 morphological forms-
- Trophozoite
- Pre-cyst
- Cyst – uninucleate, binucleate, and quadrinucleate
Trophozoite
- It is the growing or feeding stage.
- Only form is present in the tissue.
- It usually appears only in diarrheic feces and survives only for few hours.
- It exhibits slow gliding movement with pseudopodium and having a shape that is not fixed due to constantly changing position.
- Its size is 10-60μm (20-30μm avg.).
Pre cystic stage - Smaller in size (10-20μm in diameter)
- Oval with blunt pseudo podium projecting from the periphery
- Endoplasm is free of ingested RBC and other food particles.
- The nucleus is relatively large but retains the characteristic of trophozoite.
Cyst
- It may be uninucleate, binucleate, and quadrinucleate.
- Mature cyst- quadrinucleate with spherical shape
- Size – a. small – 6-9μm
b. large – 12-15μm - Cyst begins as uninucleate body soon divides by binary fission and develops into binucleate and quadrinucleate.
Life Cycle of Entamoeba histolytica
Entamoeba histolytica Passes life cycle in only one host i.e. Man
2 phases of development-trophozoite and cyst with the transitory stage of pre cystic phase
Infective form- mature cyst (Quadrinucleate cyst)
Mode of infection – feco-oral route
Site of localization– large intestine (caecum)
Pathogenesis of Entamoeba histolytica
Infective stage- mature quadrinucleate cyst
The reservoir of infection- human
Mode of infection- fecal-oral route
1. fecal contamination of drinking water, vegetables, and food
2. eating of uncooked vegetables and fruit which have been fertilized with infected human feces
3. handling of food by infected individuals (cyst passers or cyst carriers)
Incubation period– 4-5 days
Pathogenic lesion-
a. primary or intestinal – infection is entirely limited to LI
b. secondary or extraintestinal or metastatic lesion
Intestinal ulcer
Site – lesions may be
a. Generalized-whole length of LI up to internal sphincter is involved
b. Localized
Ileocecal region- commonest site
Sigmoido-rectal region
Shape – flask-shaped ulcer
Ulcers maybe
a. superficial-up to muscularis mucosa
b. deep- into the submucous layer-
Extraintestinal lesion
- Almost always precede by intestinal amoebiasis whether symptomatic or asymptomatic
- Due to the migration of trophozoites from the ulcer site
Clinical manifestation
- Amoebic colitis
- Gradual in onset, with symptoms presenting over 1-2 weeks
- Patients typically present with cramping abdominal pain, watery or bloody diarrhea, and weight loss or anorexia.
- Fever
- May mimic acute appendicitis.
Fulminant amoebic colitis
- It is a rare complication of amoebic dysentery (< 0.5% of cases).
- Presents with the rapid onset of severe bloody diarrhea, severe abdominal pain, and evidence of peritonitis and fever.
- Predisposing factors include poor nutrition, pregnancy, corticosteroid use, and very young age (< 2 years).
- Intestinal perforation is common.
Chronic amoebic colitis
It is clinically similar to inflammatory bowel disease (IBD). There is recurrent episodes of bloody diarrhea and vague abdominal discomfort.
Amebomas
It is a less common form of intestinal disease, arises from the formation of annular colonic granulation in response to the infecting organisms, which results in a large local lesion of the bowel.
Amoebic peritonitis
It is generally secondary to a ruptured liver abscess. Patients present with fever and a rigid distended abdomen. Amoebic appendicitis in countries of high prevalence, amoebiasis occasionally presents as acute appendicitis.
Laboratory diagnosis of Entamoeba histolytica
It is divided into two parts. One is a diagnosis of intestinal amoebiasis whereas another diagnosis of extra intestinal amoebiasis.
Lab Diagnosis of Intestinal amoebiasis
Specimen: fresh stool, colonoscopic biopsy, or scraping from the margin of the lesion
- macroscopic examination of stool
- microscopic examination
- culture – done in asymptomatic case
- antigen detection
- antibody detection
- PCR
Microscopic Examination
Method: Wet mount preparation with normal saline and iodine
permanent stain- trichrome stain, iron, and hematoxylin stain
Stool leukocytes may be found, but in fewer numbers than in shigellosis
trophozoites that contain ingested red blood cells (RBCs) – is diagnostic of E. histolytica infection
Examination of a single stool sample has a sensitivity of only 33-50%; however, examination of 3 stool samples over no more than 10 days can improve the detection rate to 85-95%.
Culture
It is common in following media like
- NIH medium
- Boeck and Drbohlav’s medium
- Robinsons medium
- Diamonds medium
Antigen detection
Enzyme-linked immunosorbent assay (ELISA) is used to detect antigens from E. histolytica in stool samples.
Antibody detection
Methods-ELISA, latex agglutination test, Indirect hemagglutination, indirect fluorescent assay, RIA, and CCIE.
Diagnosis of extraintestinal amoebiasis
- Demonstration of trophozoite in aspirate taken from a different site
- Blood examination
- Antibody detection
- Molecular test- PCR, DNA probe
- Intradermal test
- Radiological examination- chest X-ray, USG, CT scan, MRI
Blood tests
- Leukocytosis-15,000-30,000/cu mm (>75% neutrophils)
- Elevated alkaline phosphatase level and SGOT level.
- Mildly elevated bilirubin level
Treatment of Entamoeba histolytica
Tissue amebicides
intestinal wall, liver, and other metastatic lesions: emetine, dehydroemetine-parenteral
Liver and lungs only: 4-aminoquinolone ( chloroquine)
Luminal amebicides
Direct-acting:
i) halogenated hydroxyquinolones-diodoquin, clioquinol
ii) Dichloroacetamide group- diloxanide
iii) Antibiotics-paromomycin ( brand name humatin -oral)
b. Indirect acting-tetracycline
Both luminal and tissue amebicides: oral Metronidazole, tinidazole, nitroimidazole
Prophylaxis of Entamoeba histolytica
Personal prophylaxis:
- Use of boiled drinking water
- Protection of food and drink from flies, cockroaches, and rats
- Not eating raw vegetables and fruits
- Personal cleanliness and elementary hygiene
Community prophylaxis:
- Effective sanitary disposal of feces
- Protection of water supplies from fecal contamination
- Avoidance of the use of human excrement as fertilizer
- Detection and isolation of carriers
About amoebic versus bacillary dysentery, click on this title.
Further Readings
- Isenberg clinical microbiology procedures Handbook
2nd edition. Vol. 2 - Merkell and Voge’s medical parasitology
9th edition. - Parasitology: 12th edition
By K. D. Chatterjee - District laboratory practice in Tropical countries –Part-I.
By Monica Chesbrough. - Medical Parasitology by Abhay R. Satoskar, Gary L. Simon, Peter J. Hotez and Moriya Tsuji
- Atlas of Medical Helminthology and protozoology -4th edn -P.L. Chiodini, A.H. Moody, D.W. Manser