

Patient history
A well educated and high profile patient with the age of 53 years old having a history of Chronic Suppurative Otitis Media (CSOM) suffering for more than three months; visited many clinicians in clinics to even hospital; used antibacterial drugs but didn’t get benefited and finally he had to come to a tertiary care hospital in the department of ENT & HNS OPD. The doctor observed his ear with an otoscope and said you were infected with fungus and so he suggested for culture and sensitivity of aural discharge and follow after a week for further treatment.
Sample collection
We received four samples from right ear discharge for the following purposes-
first aural swab inoculated into Robertson’s cooked meat medium (RCM), second swab into Subouraud Dextrose Agar (SDA) at the collection site, and remaining third inoculated into Chocolate agar, blood agar and MacConkey agar and fourth swab for Gram staining and KOH preparation respectively. All the procedures were performed with standard protocols.
Laboratory Diagnosis of Aspergillus
Findings:
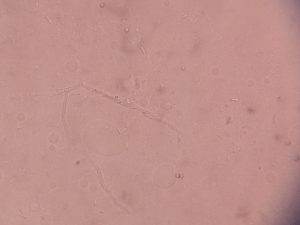
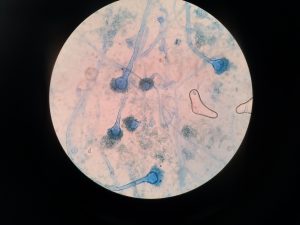
Potassium Hydroxide (KOH) Preparation– Septate fungal elements seen
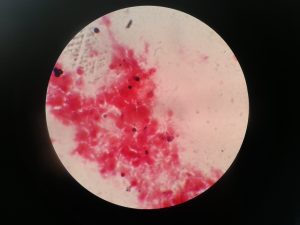
Gram staining– Pus cells plenty, Fungal spores but no bacteria seen
After 24 hours of incubation-
Chocolate agar- no bacterial growth
Blood agar- no bacterial growth
MacConkey agar-no bacterial growth
Note: Fungal growth emerging in all three plates observed.
After 48 hours of incubation-
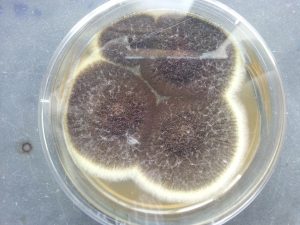
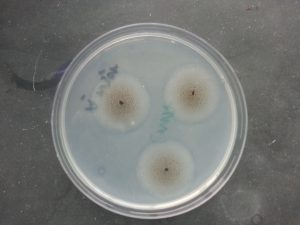
SDA with fungal growth and was further inoculated into a cornmeal agar(CMA) and both are further incubated.
after 72 hours of incubation,
Lactose Phenol Cotton Blue (LPCB) tease mount performed from these two media-
Aspergillus structures were found from both
After 72 hours, RCM was further subcultured into Blood agar having discs of Metronidazole and gentamycin; and incubated for 48 hours anaerobically.
No bacterial growth but light growth of fungus seen
LPCB tease mount suggestive of Aspergillus structures
Result
Aspergillus niger isolated
(Note- Antifungal Sensitivity Testing was not performed )
Final Impression
We generally ignore fungal infection but here Aspergillus niger is only an aetiological agent and after antifungal medication, the patient gets cured.
Diagnosis is the third eye that is why we have to observe from this angle too.
Supporting images:





Further Reading
- Medical Mycology. Editors: Emmons and Binford, 2nd ed 1970, Publisher Lea and Febiger, Philadelphia.
- Rippon’s JW: Medical Microbiology. The pathogenic fungi and the Pathogenic Actinomycetes. 3rd ed 1988 Publisher WB saunder co, Philadelphia.
- Clinical Microbiology Procedure Handbook Vol. I & II, Chief in editor H.D. Isenberg, Albert Einstein College of Medicine, New York, Publisher ASM (American Society for Microbiology), Washington DC.
- A Text-Book of Medical Mycology. Editor: Jagdish Chander. Publication Mehata, India.
- Practical Laboratory Mycology. Editors: Koneman E.W. and G.D. Roberts, 3rd ed 1985, Publisher Williams and Wilkins, Baltimore.
- Topley & Wilsons Medical Mycology. Editors: M.T. Parker & L.H. Collier, 8th ed 1990, Publisher Edward Arnold publication, London.
- Textbook of Diagnostic Microbiology. Editors: Connie R. Mahon, Donald G. Lehman & George Manuselis, 3rd edition2007, Publisher Elsevier.
- Mackie and Mc Cartney Practical Medical Microbiology. Editors: J.G. Colle, A.G. Fraser, B.P. Marmion, A. Simmous, 4th ed, Publisher Churchill Living Stone, New York, Melborne, Sans Franscisco 1996.
- Bailey & Scott’s Diagnostic Microbiology. Editors: Bettey A. Forbes, Daniel F. Sahm & Alice S. Weissfeld, 12th ed 2007, Publisher Elsevier.